Here are a bunch of little bites to satisfy your hunger for movie culture:
Character Resurrection of the Day:
Daniel Stern reprises his Rooke of the Year role of Coach Phil Brickma for a couple videos on YouTube. See more at /Film.
[embedded content]
Movie Takedown of the Day:
In case you need more reason to dislike it, Honest Trailers goes biblical on X-Men: Apocalypse:
[embedded content]
Alternate Ending of the Day:
Suicide Squad also takes more beatings with this animated parody and suggestion for how it should have ended:
[embedded content]
Vintage Image of the Day:
Andrzej Wajda, who died Saturday, filming Jerzy Radziwilowicz and Krystyna Janda for Man of Iron, which was released in the U.S. on this day 35 years ago:
Filmmaker in Focus:
Jacob T. Swinney spotlights Nicolas Winding Refn’s use of mirrors and characters’ reflections in his movies:
[embedded content]
Actor in the Spotlight:
Learn all about Ben Affleck and how he started acting in his childhood in ScreenCrush’s You Think You Know Movies?:
[embedded content]
Film History Lesson of the Day:
Frame by Frame looks at the scary origins of found footage horror movies, going back much further back than The Blair Witch Project to Italy’s Mondo and cannibal films:
[embedded content]
Video List of the Day:
One Perfect Shot counts down the best shots in horror movies, including The Exorcist and The Shining, just in time for Halloween:
[embedded content]
Adorable Cosplay of the Day:
Also ready for Halloween is this little girl dressed as Holtzman from the new version of Ghostbusters (via Paul Feig):
Comcast has been fined $2.3 million by the Federal Communications Commission for charging customers for equipment or services they never ordered. Tali Arbel/APhide caption
toggle caption
Tali Arbel/AP
Cable giant Comcast Corp. has been ordered by federal regulators to pay $2.3 million for wrongfully charging customers for gear and services they never requested. Officials say it is the largest civil penalty imposed on a cable operator.
On Tuesday, the Federal Communications Commission ordered Comcast to pay the fine after investigating complaints that some customers were charged for equipment such as set-top boxes, and services such as premium channels even after they had specifically rejected offers from Comcast representatives.
The fine was announced in a statement issued by the chief of the Enforcement Bureau at the FCC, Travis LeBlanc.
“It is basic that a cable bill should include charges only for services and equipment ordered by the customer—nothing more and nothing less. We expect all cable and phone companies to take responsibility for the accuracy of their bills and to ensure their customers have authorized any charges,” said LeBlanc.
The company agreed to make it easier for customers to know what equipment or services are on their account and to simplify the process for disputing charges.
Comcast acknowledged that “in the past, our customer service should have been better and our bills clearer, and that customers have at times been unnecessarily frustrated or confused.”
But in a statement, the company defended itself saying that the FCC “found no problematic policy or intentional wrongdoing, but just isolated errors or customer confusion.”
Matt Larson, shortly after his brain surgery, with his wife Kelly. Larson says he would like the option to end his life rather than face a painful death. Courtesy of Matt Larsonhide caption
toggle caption
Courtesy of Matt Larson
Last spring everything changed for Denver resident Matt Larson.
“One day I was fine,” says Larson. “The next I was being rushed by ambulance to Denver Health following two very massive and violent seizures.”
The force of the seizures, from the sheer shaking, fractured and dislocated his shoulders and snapped two bones in his back. Soon his providers had life-altering test results.
“They came back and shut the door and said ‘you have mass on your brain,’ which was tough to hear,” says Larson.
The diagnosis, a malignant brain tumor called an anaplastic oligodendroglioma, rocked his world. Larson, 36, and his girlfriend, Kelly, decided to get married. He says a couple of days later, surgeons cracked open his skull and scooped out part of his brain. Since then he’s endured the tough road of radiation and chemo, with a sobering outlook.
“I have a 50/50 probability that I’m going to live,” says Larson. “I hope to beat the odds. I desperately want to live.”
But Larson has decided that if the brain cancer returns and is incurable, he’d like the option to end his life rather than face the possibility of an agonizing and painful death.
“It would just bring me a ton of peace and comfort now to know that I have this option,” Larson says.
He’s become an advocate for Colorado’s Proposition 106. It would give mentally competent adults the ability to end their lives with a doctor-prescribed drug, generally a sleeping medication called secobarbital.
“We need to help people diminish and assuage their suffering any way we can,” says Dr. David Grube, a family doctor in Oregon, one of five states to allow the practice.
Grube, who retired after practicing for 38 years, is also national medical director for the group Compassion & Choices. He became a proponent of what he calls “death with dignity” shortly before the law passed in Oregon in 1994. He was moved to the position after one of his patients, who was dying from bladder cancer, shot himself to death.
“If I can ever prevent such a violent and tragic end to a person’s life, I should be open to helping people,” Grube says.
Five states — Washington, Oregon, California and Vermont — currently allow the practice. Montana has effectively legalized it, due to a court ruling that protects doctors who help dying patients from prosecution.
Colorado’s proposal is modeled after Oregon’s law. In both, two doctors must determine a patient is mentally capable of making the choice and isn’t under undue influence or coercion. Grube says he has helped about 30 people end their lives, with about a third of those who requested medications deciding not to take them.
“Many more people just want to talk about it, just want to know if it’s a possible option,” says Grube. “Still, in all, it’s quite uncommon.”
According to the Oregon Public Health Division, during 2015, 218 people received prescriptions for lethal medications under the provisions of the state’s Death With Dignity Act. That was up from 155 the prior year. The division has received reports of 132 people who died in 2015 from taking the medications prescribed under the act, a rate of 38.6 per 10,000 patients.
More than 90 percent of those patients died at home and were enrolled in hospice care. Since the Oregon law was passed, 1,545 people have received legal prescriptions; 991 patients died ingesting the medications.
When patients were asked why they decided to consider ending their lives, the most common concerns were that they were less able to engage in activities that make life enjoyable, and that they were losing both autonomy and dignity. Further down the list was inadequate pain control and the financial impact of the treatment.
Doctors As Healers
But Denver physician Alan Rastrelli opposes the proposal. He worries it will erode the public’s trust in doctors as healers.
“Physicians will go towards this philosophy of assisting a patient in their death,” he says. “That will destroy, I think, the patient and physician relationship.”
Dr. Alan Rastrelli, a hospice and palliative care physician, says Proposition 106 will erode the doctor-patient relationship. John Daley/CPRhide caption
toggle caption
John Daley/CPR
Rastrelli, who practiced anesthesiology for 28 years, transitioned into hospice and palliative medicine 15 years ago. He says when doctors help patients end their lives it creates a societal and bioethical calamity.
Rastrelli worries about what the initiative doesn’t do, such as require a physician to be present when the person dies. He also said it’s difficult to know about common problems or mistakes are because reporting requirements in Oregon, and in Colorado’s proposal, are weak.
He advocates helping dying patients to use pain relievers and receive spiritual and psychological support to ease suffering.
“Woody Allen said, ‘I’m not afraid of dying, I just don’t want to be there when it happens,’ ” Rastrelli says. “We can help people be okay all the way through to the end.”
That makes a lot of sense to advocates with Not Dead Yet, a national group run by people with disabilities that opposes the proposal.
Anita Cameron, one of the groups board members, says doctors “are humans and they make mistakes.”
Anita Cameron, a board member of the group “Not Dead Yet,” opposes Proposition 106. John Daley/CPRhide caption
toggle caption
John Daley/CPR
Cameron’s mother, Alice, was diagnosed with end-stage chronic lung disease seven years ago. She was given less than six months to live. Today, Cameron’s mother is still alive.
“Had the law been in place, I’m pretty sure those doctors would have convinced my mom to take the pills,” Cameron said. “And she’d be dead.”
Cameron has several disabilities, including multiple sclerosis. She worries the ballot proposal will encourage people with disabilities to kill themselves. She also thinks that in some cases insurers will agree to pay for end-of-life medications, but not for measures to keep someone alive.
“When is it going to be a duty to die?” asks Cameron. “That’s what euthanasia is and when is it going to stop being a choice?”
Battle Draws Big Bucks
The ballot initiative is drawing passion — and plenty of money.
According to the latest filings with the Colorado Secretary of State’s office, backers have raised about $5.3 million, mostly from Compassion & Choices Action Network.
The “No Assisted Suicide Colorado” campaign has raised $1.8 million. That money is primarily coming from the Roman Catholic Archdiocese of Denver, which has donated $1.1 million, as well as other archdioceses around the country.
Both groups have also received numerous smaller donations.
The board of the Colorado Medical Society, the state’s largest physician group, voted to take a neutral position on the measure. President-elect Dr. Katie Lozano calls the proposal “the most personal of decisions that must be left to our patients” to decide.
A February poll of 618 Colorado physicians before the ballot measure was proposed found support within the group for physician-assisted death in general. Fifty-six percent of medical society members favored it; 35 percent opposed.
Among those who frequently treat patients in later stages of a terminal illness, the gap was smaller, with 50 percent backing physician-assisted death and 41 percent opposing it.
The medical society said there was a consensus that if the law were to pass, the medical society should focus on protecting patients and doctors, and increase awareness of end-of-life choices, emphasizing the importance of palliative and hospice care.
Election ballots will start being mailed next week.
This story is part of a reporting partnership with NPR, Colorado Public Radio and Kaiser Health News.
Here are a bunch of little bites to satisfy your hunger for movie culture:
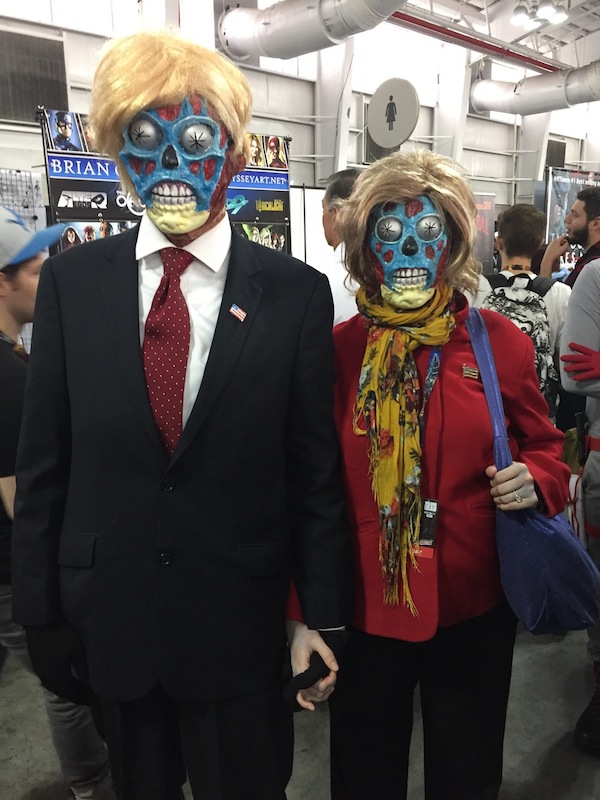
Cosplay of the Day:
For those of you still undecided about the presidential election, is it because you think both candidates are just evil aliens in disguise? This cosplay of Donald Trump and Hillary Clinton in They Live represents you (via Fashionably Geek):
Movie Scene Reenactment of the Day:
Watch Sam Neill re-create a scene from Jurassic Park with help from Miranda Hart as Ellie, John Bishop as a stand-in for the dinosaur and Ewan McGregor as the voice of the dinosaur on the Graham Norton Show (via Mashable):
[embedded content]
Animated Short Film of the Day:
Speaking of Jurassic Park, Lego and Universal joined forces for an animated Jurassic World short that is part prequel to and part reworking of the plot of last year’s hit. Watch the first part below (via /Film).
[embedded content]
Movie Marketing of the Day:
This banner for Doctor Strange spotted in China and tweeted by director Scott Derrickson should easily make a few heads turn and take note of what it’s selling:
Lin-Manuel Miranda hosted Saturday Night Live over the weekend and performed in a parody of The Music Man that satirizes the current Wells Fargo controversy:
Vintage Image of the Day:
Ed Wood, who was born on this day in 1924, with Bela Lugosi on the set of 1953’s Glen or Glenda?:
Celebrity Film Analysis of the Day:
Julie Delpy selects, watches and analyzes Martin Scorsese’s After Hours in this Academy Originals video:
[embedded content]
Video Essay of the Day:
Now You See It looks at geometry in the film frame with particular focus on animation and the use of round and angled shapes to represent good and evil:
[embedded content]
Classic Trailer of the Day:
Today is the 30th anniversary of the release of Peggy Sue Got Married. Watch the original trailer for the time-travel movie below.
Samsung says it is suspending production of the Samsung Galaxy Note 7 after reports that its batteries overheat and catch fire. The U.S. government recommends powering down and not using the device even if it is a replacement phone. Richard Drew/APhide caption
toggle caption
Richard Drew/AP
Updated 9:50 p.m. ET with FAA statement
There’s more bad news for Samsung Electronics as the South Korean company was trying to solve the problem of its flagship Galaxy Note 7 smartphone catching fire. Samsung, the global leader in smartphone production, announced that it is suspending sales of the smartphone after reports that some replacement devices were also spontaneously igniting.
The U.S. Consumer Product Safety Commission issued a statement advising “all consumers who own a Samsung Galaxy Note7 to power them down and stop charging or using the device.”
“Samsung is being squishy on the details. Samsung says in a statement that ‘we are readjusting our supply,’ without specifying if it’s [the] supply of batteries or another phone part.”
The New York Times reported that the company hoped to provide an update within a month.
“Samsung made the decision to halt production for consumer safety reasons and in cooperation with the authorities in the United States and China, according to the person familiar with the process.”
The news comes after Samsung announced last month that it would recall 2.5 million Galaxy Note 7 smartphones amid reports that batteries were overheating and were a safety risk. The company reportedly changed battery suppliers, but that doesn’t appear to have solved the problem. Last week, a Samsung Note 7 began smoking on a Southwest Airlines flight, prompting an evacuation of the plane. The phone was reported by the owner to be a replacement phone.
The four top U.S. telecom companies, Verizon, AT&T, T-Mobile, and Sprint have announced that they will no longer sell the replacement version of the Note 7. All four are offering to replace existing Note 7 phones.
Australia’s top three telecoms—Telstra, Optus and Vodafone Australia—also announced that they would no longer ship the Note 7.
Among technology publications and writers, the question now is, how much damage will the battery malfunction do to Samsung’s reputation?
The chief analyst at Jackdaw Research, Jan Dawson told Wired:
“This is the worst-case scenario for Samsung. Now that the replacement devices seem to be having the same problems, it calls into question Samsung’s whole product testing methodology and its scrutiny of its suppliers. That’s much worse than a one-off.”
Here’s what the chairman of Reputation Management Consultants, Eric Schifffer told Reuters:
“If the Note 7 is allowed to continue it could lead to the single greatest act of brand self-destruction in the history of modern technology. Samsung needs to take a giant write-down and cast the Note 7 to the engineering hall of shame next to the Ford Pinto.”
Mylan CEO Heather Bresch holds up an EpiPen two-pack while testifying about price increases to the House Oversight and Government Reform Committee on Sept. 21. Pablo Martinez Monsivais/APhide caption
toggle caption
Pablo Martinez Monsivais/AP
Three doctors who have led a task force that evaluates preventive medical services say the group’s recommendations shouldn’t be tied by law to insurance coverage.
The former chairmen of the U.S. Preventive Services Task Force say the link between medical recommendations and insurance coverage leads to financial incentives that can corrupt the process and distort people’s health care decisions.
Under the Affordable Care Act, any preventive service that receives one of the USPSTF’s top two ratings must be covered by insurance without any out-of-pocket cost for the patient. The doctors advice to decouple the task force ratings from insurance coverage would require a change in the health law.
The authors of the commentary, which appears Monday in the Annals of Internal Medicine, point to heavy lobbying by the pharmaceutical company Mylan N.V. to get its anti-allergy device EpiPen deemed a preventive service. They say such lobbying can interfere with the task force’s mission to evaluate medical services to improve the health of the overall population.
“When people try to twist that mission for their own purposes, essentially what they’re doing is violating the integrity of the task force process, and it’s distracting from the mission,” says Dr. Virginia Moyer, the lead author of the commentary. Moyer, a former chairman of the task force, is now a vice president of the American Board of Pediatrics.
The USPSTF is an independent group of volunteer physicians who review the research on preventive medical services, such as vaccines and screenings tests, and recommend who should get them and how often.
Mylan has been lobbying the task force to have the EpiPen listed as a preventive device, even though it is used by people with diagnosed allergies. The EpiPen is an automatic injector that delivers a dose of epinephrine to stop dangerous allergic reactions. A two-pack costs more than $633, according to GoodRx.
The company has been under fire in recent months because it has raised the price of the device more than fivefold since 2007, even though the product has been on the market for decades. Mylan CEO Heather Bresch has blamed the uproar on trends in insurance coverage that leave patients responsible for a larger share of their medical costs.
If EpiPens were covered as preventive medications, patients could get them at no cost. The price increases Mylan has put in place would be invisible to consumers but would have to be borne by insurers.
“What Mylan has done, or what they’re attempting to do with this effort, is use a provision in law, which is intended to give people access to preventive services, and use it to their advantage for something that just plain is not a preventive service,” Moyer says.
That effort by Mylan, which was detailed in a story by The New York Times, spurred Moyer and her two colleagues, Dr. Michael LeFevre and Dr. Ned Calonge, who were also task force leaders, to write the opinion piece that questions the overall idea that insurance coverage should be tied by statute to the recommendations of the volunteer medical group.
The authors say the issues with the link go beyond the problem of lobbying. By putting prevention ahead of treatment of illness by making it free of cost, the system created by the ACA may be making treatment of illness more expensive and putting it out of reach of some patients.
“If such financial access comes at the cost of increased deductibles or copays for equally important services that are not preventive, then we must question whether the link inadvertently discourages other important care,” they write.
“Perhaps it is time for the USPSTF to inform, but not determine, coverage,” they conclude.
A recent survey by the Kaiser Family Foundation shows that more than half of people with insurance through their employer have policies with deductibles of more than $1,000.
Many advocates and economists agree that preventive services can cost more but also can improve the quality of health care. When the Affordable Care Act was being debated, advocates on both sides argued whether or not preventive services would save money in the long run.
“Preventive health services have become quite expensive over time,” says Joe Antos, a resident scholar at the American Enterprise Institute.
He says some preventive services such as vaccines are inexpensive and undoubtedly valuable. Others, such as mammograms, are also medically important but don’t necessarily save money.
When those services are provided free, the costs are spread across all policy holders through premiums and deductibles.
But Antos cautions against blaming rising deductibles and premiums only on preventive care.
“To what extent have preventive services been responsible for the big increase in deductibles and co-payments over the last decade or so?” he asks. “I would argue that they’ve contributed. But we’re really talking about rising health care costs, not just preventive services.”
In light of a recent rash of “creepy clown” sightings and incidents across the country, some working clowns say the controversy is negatively affecting their business.
MICHEL MARTIN, HOST:
This next story falls under the category of funny-not-funny. If there are school-age children at your house, you’ve probably gotten wind of stories involving creepy clowns. In some two dozen states, police have reported calls claiming that creepy clowns were actually lurking in public places, causing school lockdowns in some cases. Now, most of these reports have since been debunked as hoaxes, but a few arrests have been made. And as NPR’s Alexi Horowitz-Ghazi reports, the creepy clown scare is anything but amusing for those in the funny business.
ALEXI HOROWITZ-GHAZI, BYLINE: When you ask Mr. Rainbow of Durham, N.C. how he became a professional clown, he’ll blame it on his wife.
DAVID BARTLETT: It’s my wife’s fault, yes. She signed me up for a class in balloon sculpting that I didn’t want to go to. And because we couldn’t get our money back, I went to the class.
HOROWITZ-GHAZI: David Bartlett, as he’s known off the clock, quickly found he had a knack for clowning around, so he quit his job as a schoolteacher to go full-time. Every week, he performs at hospitals, office parties, colleges. And what has working almost 3,000 birthday parties taught him?
BARTLETT: It doesn’t matter what you do. It doesn’t matter what you have in your hands. The art of the clown is to take whatever you do and make people laugh.
HOROWITZ-GHAZI: Bartlett says he’s used to dealing with coulrophobia, or the fear of clowns. It’s part of the job. And he isn’t too worried about the latest round of scary clown sightings.
BARTLETT: It’s not affecting my business model because I’m a hometown clown in an area where they’ve known me for many years.
HOROWITZ-GHAZI: But many working clowns are taking the scare a little more seriously.
MIKE WESLEY: I haven’t done a show since this began.
HOROWITZ-GHAZI: Mike Wesley is a retired mailman and part-time clown known as Mr. Funny Bunny in central Ohio.
WESLEY: People started calling me up and saying they’ve had second thoughts, and what else can I do?
HOROWITZ-GHAZI: He says that over his three decades in the industry, he’s watched similar panics come and go every few years.
WESLEY: And they are timed to things that involve clowns in the news.
HOROWITZ-GHAZI: Like the case of John Wayne Gacy in the late 1970s, the serial killer who painted prison portraits of himself dressed as a clown. Or movies like “IT,” based on Stephen King’s novel about an evil clown named Pennywise.
(SOUNDBITE OF FILM, “IT”)
TIM CURRY: (As Pennywise) I am your worst dream come true. I’m everything you ever were afraid of.
HOROWITZ-GHAZI: Mike Wesley says that past frenzies would typically blow over in a couple weeks, but that social media has spawned copycats around the country. And that’s made things difficult for people who clown to keep the lights on.
LORI HURLEY: I am Half-Pint, my husband is Oscar, and my children are Teaspoon, Little Squirt and Thumper.
HOROWITZ-GHAZI: Lori Hurley and her family are professional clowns in St. Paul, Minn.
HURLEY: Because I’m a clown, I can see the bright side and the humor in anything. But there is a real problem when people can’t distinguish the difference between the real clowns and people who dress up as clowns with the intent to scare.
HOROWITZ-GHAZI: She says business is down around 20 percent since the sightings started.
HURLEY: And when we have people call and cancel bookings, it hurts my family. When I’m driving down the road as a clown and people are looking at me like I’m that bad, evil, scary clown and they’ve just heard on the radio how they should take matters into their own hands, suddenly my safety is jeopardized, as is my children.
HOROWITZ-GHAZI: Hurley recently came across a photo circulating on social media of a fake clown hunting permit which reads, also valid for al-Qaida, Taliban and Boko Haram.
HURLEY: When you start putting clowns up there with terrorists, then I think people need to take a step back and ask themselves, yeah, maybe it was funny in thought, but is it really funny? Because underneath the makeup – for the real clowns – are real people with real families, with real jobs.
HOROWITZ-GHAZI: Mr. Rainbow, aka David Bartlett, on the other hand, says this, too, shall pass. And his advice to fellow working clowns?
BARTLETT: Make them laugh. Go back to the basics of what clowning is, and they will know who you are.
HOROWITZ-GHAZI: Well, you heard the clown. Alexi Horowitz-Ghazi, NPR News.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
The study looked at the relationship between women who used hormonal birth control, and antidepressant use, and diagnoses of serious depression. AJPhoto/Science Sourcehide caption
When the birth control pill debuted more than 50 years ago, women wanted to know: Is it safe? There wasn’t much evidence to answer that question, but women embraced the Pill as a revolutionary improvement in contraception.
Today, millions of women around the world use hormonal contraceptives that have expanded beyond the Pill to patches, implants, injections and uterine devices. Decades of research support their safety, and serious but very rare side effects such as blood clots are finally much better understood. But other areas of research lag, and we still don’t know as much as we’d like about how these medications affect women’s mental health.
So when a study came out linking hormonal birth control and depression, the headlines went wild. The stories made for good clicks, but not so great science reporting. Insufficient skepticism about a single study makes it easy to imply birth control definitely causes depression when the study shows nothing of the sort.
The study, which was conducted in Denmark and published in JAMA Psychiatry, analyzed 14 years’ worth of health data for more than 1 million women from national healthcare systems and databases not available in most other countries. It also measured depression two ways: diagnosis at a psychiatric hospital, which would be quite severe depression, or filling a prescription for antidepressants. Across the whole study, 2 percent of all women ages 15 to 34, were diagnosed with depression at a hospital and 13 percent began taking antidepressants.
Several news stories reported an 80 percent increase in risk of depression in some groups of women, but few noted that was relative risk, which is an expression of proportional increase. An 80 percent relative risk does not mean that 80 percent of women taking hormonal birth control develop depression. It means that if 10 women not taking hormonal birth control develop depression, then 18 women on the birth control will develop depression.
In this study, that 80 percent increase in relative risk referred specifically to the likelihood that those ages 15 to 19 taking combined oral contraceptives — the pill containing both progestin and estrogen — would begin taking antidepressants after going on birth control.
However, looking at absolute risks conveys a less dire interpretation. Among women not taking hormonal birth control, 1.7 percent took antidepressants and 0.28 percent received a depression diagnosis at a psychiatric hospital. By comparison, 2.2 percent of women who started birth control began taking antidepressants afterward, and 0.3 percent were diagnosed with depression at a hospital. Basically, about 0.5 percent of women who began hormonal contraception developed depression who might not have otherwise.
“Therefore for an individual woman, even one using a method of hormonal contraception, the overall probability of experiencing one of these outcomes in this study was still fairly low, particularly for diagnosis of depression,” explains Chelsea Polis, a senior research scientist at the Guttmacher Institute.
Rates of those filling antidepressant prescriptions were higher for other forms of hormonal birth control: 4.1 percent for the patch and 3.2 percent for the vaginal ring in the first year, for example. Psychiatric depression diagnoses occurred in 0.7 percent of patch users and 0.6 percent of vaginal ring users.
Even in terms of relative risk, though, many of the risk increases were modest: Among all women taking the combined pill, the increased risk was 10 percent for depression diagnosis and 20 percent for using antidepressants after statistically adjusting for women’s age, educational level, weight and history of endometriosis or polycystic ovary syndrome, all factors that could influence depression risk.
Other increased risks ranged from 20 to 70 percent for all women, depending on contraception type. The largest increases — up to triple the likelihood of starting antidepressants — occurred among teens using the ring or patch.
Another thing to consider is that these numbers represent correlations — two things occurring at the same time that may or may not be linked.
“Depression is common. Contraception use is common. So both of those things are commonly going to occur together,” explains Jeffrey Jensen, a professor of reproductive & developmental sciences and director of the Women’s Health Research Unit at Oregon Health & Science University in Portland.
The study used several methods to reduce the possibility that other things could be causing depression. Jensen pointed out that women who are more likely to take hormones for contraception would probably also be more likely to take antidepressants for depression, but the authors did a separate analysis to compare women to themselves before and after beginning contraception and still found a depression risk.
None of this means that birth control does not cause depression, but it doesn’t mean it does, either. Since a half percent of millions of women taking birth control adds up, it’s important to know whether such a large number of women could be more susceptible to depression, which can be a very serious illness, after starting hormonal contraception.
But it’s complicated, and subtle.
For example, the study also found that depression risk peaked six months after women began using contraceptives, but then decreased to the point that women using hormonal contraception for four years actually had lower rates of depression than those not taking it. Though this likely resulted from many women with depression stopping their birth control, those findings match up with a previous large study finding a protective effect against depression with hormonal contraception. But the studies were done differently: The earlier study included only sexually active women, unlike the new study.
“Unfortunately, the analysis did not provide information on the frequency of depression diagnoses or antidepressant use among women using nonhormonal methods of contraception, such as copper IUDs,” says Polis. “Such a comparison would help to clarify whether the associations were related to other factors common to women choosing to use contraception, rather than being specifically related to the hormonal content of certain contraceptive methods.”
For example, those who become sexually active in adolescence have a higher risk for depression and anxiety, as previous research has shown. Even among women in their 20s and 30s, the decision to begin hormonal contraception may accompany various other circumstances in their lives that could potentially increase the risk of depression or anxiety — not a stretch when the study identifies just a half percent of women with the increased risk.
But the possibility that sexual initiation might come with mental health risks baffled study co-author Lidegaard. “Sexual relationships are a good experience for the majority of women, so I cannot see why women would get depressed by starting sexual relationships,” Lidegaard said in an interview. He pointed out that women not in relationships may experience loneliness, a risk factor for depression, but when asked about single women having sex, he said he believes “the majority feel more happy by realizing how wonderful sexual experiences can be. Why should women get depressed from that?”
What this study does do is suggest that women may respond differently to hormones and medical treatments.
“Doctors should perhaps be more careful when they prescribe hormonal contraception to young women and get a history of previous depression first,” Lidegaard says.
There’s no question that women are going to respond differently to hormonal contraception. But those differences are not well understood.
“We’re all very, very different, and we’re moving in the direction of precision medicine,” adds Catherine Monk, an associate professor of psychiatry and director of research at the Women’s Program at Columbia University Medical Center. “There are some women who are just much more sensitive to these hormone changes.”
The higher risk of depression found among teenage girls, both Monk and Lidegaard pointed out, might be biological, since teens may be more sensitive to the hormonal changes happening during puberty.
“You need to know yourself and be really informed,” Monk says. “If I were of an age and reading this article right now, I would want to be thinking, ‘Who am I? Am I sometimes who has moodiness around my periods?’ ” She notes the importance of each woman considering these findings in conjunction with what she knows about her own body and her own circumstances.
Philosophical differences about medicine may also influence how people interpret these findings in the absence of studies showing causation. Jensen, for example, pointed out that women in developed countries no longer see other women dying during childbirth, illegal, unsafe abortions or other devastating health effects of unplanned pregnancy, and have come to places less value the effectiveness of hormonal birth control.
“Women are more skeptical of using hormonal therapy than ever before,” Jensen says. “It’s a tragedy of the riches. If you really want to be depressed, have an unintended pregnancy.”
Toward the other end of the spectrum, Monk believes we may have gone too far in using hormones to control contraception. “Getting away from barrier methods of contraception is getting away from our bodies,” she says, and she would like to see a much larger range of options for contraception for men and women.
The fact that dissent rages over this issue points out a larger question about women’s health research.
“Understanding women’s health has been neglected, and there’s not enough research into understanding our hormones,” Monk says. “This is partially a story about women’s health research and how we need more of it.”
Rachel Martin and Mike Pesca of Slate’s The Gist podcast talk about the trend of under-performing pitchers in baseball’s post-season.
RACHEL MARTIN, HOST:
And it’s time now for sports.
(SOUNDBITE OF MUSIC)
MARTIN: It’s the playoffs – the baseball playoffs, where heroes and goats are made, or so I’m told. Mike Pesca of “The Gist” joins us from the studios of Slate in New York. Hi, Mike.
MIKE PESCA, BYLINE: Hi. The goats – let us talk of the goats.
MARTIN: The goats. OK, truth be told, I’d never heard of this expression until hours ago, but everyone tells me this is a thing. I don’t even understand what it means. Heroes and…
PESCA: …A goat? Yeah…
MARTIN: …I understand what a goat is, but I don’t understand the relevance in baseball.
PESCA: Scapegoat.
MARTIN: Oh.
PESCA: Oh, there’s so much relevance we can’t even get into. Like, there’s this curse…
MARTIN: …Oh, we can’t even get into it.
PESCA: There’s this curse of the goats with the Cubs. And GOAT is also an acronym for Greatest of All Time. But we’re going to talk about the goats who are the heels, the guys who let their teams down.
MARTIN: OK, so there’s two pitchers who are getting a lot of attention right now. Who are they?
PESCA: Yes, David Price and Clayton Kershaw, two of the best pitchers. I should say that Clayton Kershaw of the Dodgers is just the best pitcher in baseball. He’s 28 years old. He’s going to the Hall of Fame. Right now, he’d probably make the Hall of Fame, actually, even if he quit tomorrow. And David Price is also a great pitcher. To give you some idea of how great they are, Clayton Kershaw gets paid $34 million a year, David Price $30 million a year.
And yet when it comes to the big stage both of these guys, to varying degrees, are disappointing. And it happened in the first game that each of them pitched in the playoffs. Especially David Price, a guy getting paid $30 million dollars a year, you’d hope he could get out of the fourth inning. But he couldn’t, once again letting his team down. Whereas Kershaw just wasn’t his normal dazzling self. But he does have a history in the playoffs of sometimes getting bombed.
MARTIN: So is that just ’cause it’s the playoffs and there’s a lot of pressure? I mean, but – what’s the deal?
PESCA: OK, I think there are two different guys, two different explanations. I think first of all, Kershaw is being compared to his usual regular-season self. And here’s a guy who has, you know, 170 strikeouts in a year and 11 walks – just spectacular. So if he pitches only pretty good in the playoffs in his first game – seven innings, three runs – that’s pretty good. We’re going to say a little disappointing. And the couple of games where he was really bad, which were a couple playoff games against the Cardinals – gave up big home runs – you say, what’s up with Kershaw?
Price, on the other hand, I do think something’s going on. It’s very hard to prove, but if you listen to interviews with other players or ex-players they say he’s maybe playing – trying too hard, gripping his balls a little hard, trying to be perfect. And when you try to be perfect and you aim instead of throw, bad things can happen. I think that there’s maybe enough evidence to say that David Price is mentally taking himself out of games.
MARTIN: And, I mean, these guys – just higher stakes – right? – compared to the hitters. The pitchers have to be good all the time, every time.
PESCA: Well, that’s a good – that’s a good thing to think about. A pitcher starts off with an ERA of 0 and can only get bad from there. A hitter starts off with a batting average of 0 but can only get good from there. So one swing of the bat can rehabilitate or make a hero in terms of a batter, but a pitcher has to be very good and consistent throughout. But to be fair or to be honest with David Price, he just has been a bad playoff pitcher. Although, you know, they’re down two games to nothing. If the Red Sox come back he could, you know, rewrite history. I just doubt we’ll see that. Kershaw can rehabilitate his image without any miraculous comeback. They’re up in their series.
MARTIN: Mike Pesca. He’s our own GOAT. He also hosts “The Gist.”
PESCA: Wait, the good kind, right?
MARTIN: That’s a compliment. The good kind.
PESCA: Yes, OK, thanks.
MARTIN: Greatest of All Time. Thanks so much, Mike.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
If you’re hoping to get a look at the Power Rangers in their suits, fighting off the other worldly summons of Rita Repulsa, you might be a bit disappointed by the first teaser trailer for the new movie. If, however, you’re in to teens getting super powers and learning to use them, you’ll be plenty happy.
Directed by Dean Israelite (Project Almanac), this rebooted Power Rangers changes mythology up a bit (at least if the ’90s TV show is your starting point). This time around the teenagers discover some alien technology in a cave and are imbued with mighty powers even without having to morph into their suits.
Check it out.
[embedded content]
Power Rangers will hit theaters on March 24, 2017.