After years of legislative gridlock, the victim compensation fund has been extended to ensure permanent funding for rescue workers whose jobs after the terror attacks caused health problems.
STEVE INSKEEP, HOST:
A 9/11 first responder has a chance to savor victory. President Trump signed a measure ensuring a compensation fund never runs out of money. NPR’s William Jones reports on how that moment looks to a man who fought to bring it about.
WILLIAM JONES, BYLINE: John Feal was a construction worker until his career was cut short in 2001. In the days after 9/11, he was a demolition manager at ground zero when a piece of steel crushed his leg. Part of his foot had to be amputated. And in the years since, he’s been lobbying lawmakers to approve permanent funding for first responders, whose illnesses continue to mount.
JOHN FEAL: Two-hundred and seventy-eight trips to D.C. We’ve been at this for almost two decades now because of poor leadership and bad politics.
JONES: Feal was at a congressional hearing in June. He watched on as his colleagues, some gravely ill, addressed a House committee. He remembers thinking that some lawmakers seemed disengaged, which he told his friend, the comedian Jon Stewart, just as he arrived to testify.
(SOUNDBITE OF ARCHIVED RECORDING)
JON STEWART: Your indifference cost these men and women their most valuable commodity – time.
JONES: Stewart’s comments came as an existing $7.4 billion fund was rapidly depleting, as thousands were becoming ill.
RICHARD ALLEYS: These aren’t just normal cancers; we call it cancer on steroids. They get diagnosed with stage 4. These are aggressive, aggressive cancers, and that’s why we’ve lost so many people.
JONES: That’s Richard Alleys. He was a firefighter at ground zero, and he believes Stewart’s testimony was a turning point.
ALLEYS: He just had that innate ability to put the spotlight on the legislators that could no longer hide.
JONES: After that hearing, legislation extending funding through 2092 to pass the House, but it faced a slightly stiffer opposition in the Senate, where Republicans Rand Paul and Mike Lee led a vote, questioning whether the bill was fiscally responsible. It eventually passed overwhelmingly, leaving the president to sign it into law.
(SOUNDBITE OF ARCHIVED RECORDING)
PRESIDENT DONALD TRUMP: For your entire lives, you have gone far beyond your duty to us. And today, we strive to fulfill our sacred duty to you.
JONES: After signing the bill, the president handed the pen to John Feal.
FEAL: The financial burden, it’s going to be lifted. This bill is going to help people for decades.
JONES: It ensures his almost 300 trips to D.C. will now have a lasting legacy.
William Jones, NPR News, in Washington.
(SOUNDBITE OF AMBIENT JAZZ ENSEMBLE’S “ELEVEN DAYS”)
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
For the first time, doctors have used the gene-editing technique CRISPR to treat a genetic disorder in the U.S. The patient, who has sickle cell disease, spoke with NPR about her treatment.
ARI SHAPIRO, HOST:
One of the most eagerly awaited medical experiments has begun in Nashville. For the first time, scientists have used the gene-editing technique called CRISPR to try to treat a genetic disorder in the United States. NPR is the only news organization to have learned the identity of the first patient and to talk with her. NPR health correspondent Rob Stein is here with more.
Hey, Rob.
ROB STEIN, BYLINE: Hey, Ari.
SHAPIRO: Who is this woman, and why is she undergoing this experimental treatment?
STEIN: Her name is Victoria Gray, and she’s 34 and lives in Forest, Miss., with her husband and four kids. And here’s a little bit about what she told me about herself when I met with her recently at the Sarah Cannon Research Institute in Nashville.
VICTORIA GRAY: Well, I don’t work. I’m a stay-at-home mom. But before I got too sick, I was working in the beauty department at Walgreens, and I was going to school to become a nurse. But that got put on hold for health reasons.
SHAPIRO: Tell us about her sickness. What is her condition?
STEIN: Yeah, so Victoria has sickle cell disease, and it’s a terrible genetic disease that primarily affects African Americans in the United States. And instead of having normal red blood cells – you know, the cells that carry oxygen in your body – sickle cell patients have a hard, sticky – it’s a sickle-shaped red blood cell that causes terrible bouts of agonizing pain and can cause lots of really serious health problems.
GRAY: Well, I’m high-risk for strokes, and I’m high-risk for heart attacks. And these things can happen to me in a blink of an eye. And my pain episodes can just come on out of the blue. I can just be laughing, and next minute, I’m crying, you know, in some of the worst pain that you could ever imagine. It’s a heavy load to carry, you know?
SHAPIRO: That sounds really tough. So how are doctors trying to use CRISPR to help people like Victoria Gray?
STEIN: Right, so this is how it works. The doctors – they take cells out of the bone marrow of sickle cell patients, and they use this CRISPR editing tool to edit a gene in those cells to turn on the production of something called fetal hemoglobin, which is usually only produced by fetuses when they’re in the womb and babies for a short time after they’re born. And then they infuse billions of these genetically modified cells from the patient back into their bodies, hopefully, to help treat their disease.
Dr. Haydar Frangoul, who’s running the study in Nashville – he explained a little bit more about how this is going to work.
HAYDAR FRANGOUL: What we are trying to do here is we are trying to introduce enough fetal hemoglobin into the red blood cell to make the red blood cell go back to being happy, squishy and not sticky and hard and can go deliver oxygen where it’s supposed to.
SHAPIRO: So she is the first sickle cell patient to get this treatment. What does it involve? What was the process like?
STEIN: Yeah, so parts of it were really pretty hard. She had to go through chemo, first of all, to wipe out her own bone marrow to make room for these CRISPR-edited cells. And then Dr. Frangoul infused more than 2 billion of those gene-edited cells into her body, and this was just a few weeks ago.
GRAY: They had the cells in a big syringe, and when it went in, my heart rate shot up real high. And so that was a little scary, tough moment for me. And just after that, I cried, but it was happy tears.
STEIN: What was that feeling like?
GRAY: It was amazing. You know, it was kind of overwhelming after all that I had went through to finally, you know, get what I came for.
STEIN: And Victoria – she calls her new gene-edited cells – she calls them her supercells.
Why do you call them supercells?
GRAY: Well, I have sickle cell, so just replacing it with a better S (laughter) makes it supercells.
SHAPIRO: Rob, it sounds like there’s a lot of potential here. But what are the concerns?
STEIN: Yeah, so, you know, there are always concerns about any new, experimental treatment. Is it safe? Will it work? And this is all really magnified with something that’s this new. Here’s Laurie Zoloth. She’s a bioethicist at the University of Chicago. And I talked to her about that.
LAURIE ZOLOTH: I am optimistic about the success of CRISPR. I just want it to be done carefully.
STEIN: Yeah, so they’re going to monitor her very closely, first of all to make sure the edited cells are safe, they’re not causing any health problems on their own, and then to try to get any clues to see if they might be working. And researchers are planning to study dozens of patients at medical centers in this country and in Canada, in Europe. It could take months, and maybe even years, to know how well it’s working.
And I talked to Victoria about that. She says she knows the risks and that it is a very early study, but she can’t help but hope that it helps her.
GRAY: I feel like the way everything had been, it was kind of fate. And I feel special to be the first to do it.
STEIN: And we’re going to be checking back with Victoria just to see how things are going.
SHAPIRO: That’s NPR’s Rob Stein with that exclusive story about CRISPR gene-editing technology.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
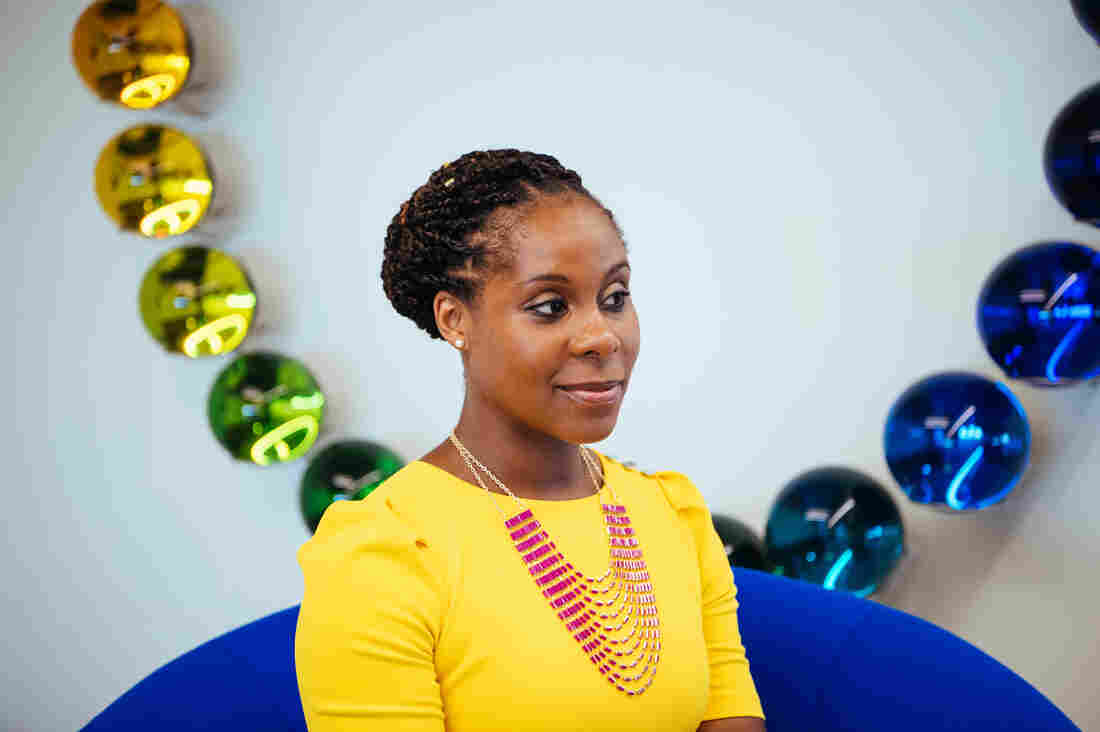
Altovise Ewing, who has a doctorate in human genetics and counseling, now works as a genetic counselor and researcher at 23andMe, one of the largest direct-to-consumer genetic testing companies, based in Mountain View, Calif.
Karen Santos for NPR
hide caption
toggle caption
Karen Santos for NPR
Altovise Ewing was a senior at Rhodes College in Memphis, Tenn., when she first learned what a genetic counselor was. Although she had a strong interest in research, she suspected working in a lab wasn’t for her — not enoughsocial interaction.
Then, when a genetic counselor came to her class as a guest lecturer, Ewing had what she recalls as a “lightbulb moment.” Genetic counseling, she realized, would allow her to be immersed in the science but also interact with patients. And maybe, she thought, she’d be able to help address racial health disparities, too.
That was 15 years ago. Ewing, who went on to earn a doctorate in Genetics and Human Genetics/Genetic Counseling from Howard University, now works as a genetic counselor for 23andMe, one of the largest direct-to-consumer genetic testing companies. As a black woman, Ewing is also a rarity in her profession.
Genetic counselors work with patients to decide when genetic testing is appropriate, interpret any test results and counsel patients on the ways hereditary diseases might impact them or their families. According to data from the U.S. Department of Labor’s Bureau of Labor Statistics, the number of genetic counselors is expected to grow by 29% between 2016 and 2026, compared with 7% average growth rate for all occupations.
23andMe’s Ewing says the lack of ethnic diversity among genetic counselors in the U.S. reduces some people’s willingness to participate in clinical trials, “because they’re not able to connect with the counselor or the scientist involved in the research initiative.”
Karen Santos for NPR
hide caption
toggle caption
Karen Santos for NPR
However, despite the field’s rapid growth, the number of African Americans, Hispanics and Native Americans working as genetic counselors has remained low.
As genetics’ role in medicine expands, diversity among providers is crucial, say people working in the field. “It is well documented that people want medical services from people who look like them, and genetic counseling is not an exception,” says Barbara Harrison, an assistant professor and genetic counselor at Howard University.
Ana Sarmiento, who wrote her master’s thesis on the importance of diversity among genetic counselors, has seen this firsthand.
“I can’t tell you how many times I’ve seen the look of relief on a Spanish-speaking patient’s face when they realize they can communicate with me,” says Sarmiento, a recent graduate of Brandeis University’s genetic counseling program. “It’s what keeps me passionate about being a genetic counselor.”
Ethnic and gender diversity among providers can also increase the depth and scope of information patients are willing to share in the clinical settings — information that’s important to their health.
“In my opinion,” says Erica Price, who just received her master’s in genetic counseling from Arcadia University, “no one fights for the black community the way other black people do. I encounter a lot of other African Americans who don’t know what genetic counseling is. But when they find out that I’m a genetic counselor, they will give me their entire family medical history.”
Bryana Rivers, who is African American, recently graduated from the University of Cincinnati’s genetic counseling program, and wrote last year about her experience with a black mother whose two children had undergone extensive genetic testing to try to determine the cause of their developmental delays.
Having a firm diagnosis, the mother explained to Rivers, could help the children get access to the resources they needed in school. The mom wanted to know if the genetic variant that had been identified in her children — one that geneticists had decided was a “variant of unknown significance” — had been observed in other black families.
That question, which she hadn’t brought up in earlier discussions with health providers who weren’t African American, led to a broader, candid discussion of what these unknown variants mean and don’t mean, and why they are more common among members of understudied minorities.
“I cannot stress enough how important it is for patients to feel comfortable, to feel heard, and to know that they will not be ignored or discriminated against by their providers based on the color of their skin,” Rivers wrote in her blog post.
“I don’t want to suggest that a genetic counselor who wasn’t black wouldn’t have listened to her, but there are factors outside of what we do and say that can have an impact on our patients. Just the fact that she was able to lower her guard a bit because we share the same racial background as her speaks volumes.”
In an interview Rivers also recounted a recent session conducted by a white female genetic counselor that Rivers was shadowing that day. The patient, who was a black woman, addressed all of her answers to Rivers, although Rivers’ official role was to merely observe the appointment.
“I do feel a responsibility as a black provider to look out for my black patients and make sure they are receiving the appropriate care,” Rivers says. “Not everyone is willing to go that extra mile, and they may be more dismissive of the concerns of black patients and may not actually hear them.”
Ewing, who also conducts research, adds that the lack of diversity among genetic counselors has had a negative impact on research.
“The lack of diversity has an effect on the willingness of minorities to pursue clinical trials, because they’re not able to connect with the counselor or the scientist involved in the research initiative,” she explains. “We are now in the era of precision and personalized medicine and we need people who are comfortable talking about genetic and genomic information with people from all walks of life, so that we’re reaching all demographics.”
In 2019, 90% of survey respondents identified as Caucasian, while only 1% of respondents identified as Black or African-American. Just over 2% of respondents identified as Hispanic, 0.4% identified as American Indian or Alaskan Native.
Some genetic counselors cite a lack of awareness among underrepresented minorities of genetic counseling as a profession as a major barrier to diversity in the field. Rivers says she had little exposure to genetic counseling as a future career path while enrolled as a biology major at the University of Maryland.
“My university stressed medical school, nursing school, or a Ph.D. in the biological sciences,” Rivers recalls. “I only had one professor in four years bring up genetic counseling.”
Samiento concurs. “You don’t have 6-year-olds running around saying ‘I want to be a genetic counselor’ — because it’s not a high visibility profession,” she says. “There are also very few minority professionals in the training programs and it takes a brave minority to look at the sea of white female faces and say ‘yes I can fit in here.’ “
“Genetic counseling is still a relatively new profession and there hasn’t been enough time and exposure for people to view [the field] the way they view other medical professions,” says Price. “People have asked me why I would pursue genetic counseling when I could be a physician assistant or a nurse or go to medical school.”
After Price’s acceptance to graduate school, one of her undergraduate professors questioned her chosen career path. “She said to me, ‘You’re a black woman in the sciences. We could have gotten you into a Ph.D. program or something where you’re making more money.’ “
As a part of its strategic plan for the years 2019-2021, the NSGC has identified diversity and inclusion as one of its four areas of strategic focus. Specific plans include developing mechanisms to highlight genetic counseling as a career in hard-to-reach communities by the end of the year. Erica Ramos, who is the immediate past president of the NSGC and serves as the board liaison to the task force, says she is optimistic that the numbers of underrepresented minorities in the field will improve.
“People in the profession have realized that we have blinders on,” she says. “But as an organization, the NSGC has been asking questions about how we can improve on diversity and be supportive of existing minority genetic counselors. We had 100 people apply to serve on the task force.”
A number of genetic counselors from diverse backgrounds have also come together to form their own support and advocacy networks. In November 2018, the Minority Genetic Professionals Network was formed to provide a forum for genetic counselors from diverse backgrounds to connect with one another.
Erika Stallings is an attorney and freelance writer based in New York City. Her work focuses on health care disparities, with a focus on breast cancer and genetics. Find her on Twitter: @quidditch424.
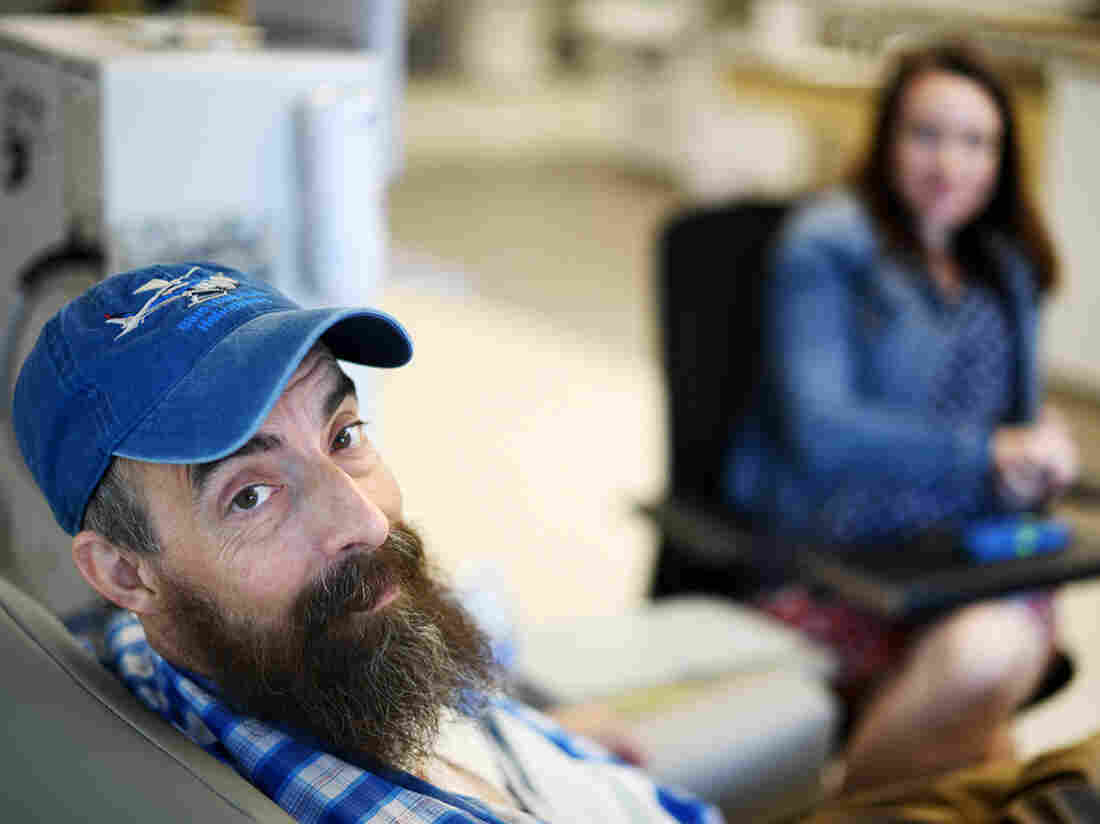
Sovereign Valentine, a personal trainer in Plains, Mont., needs dialysis for his end-stage renal disease. When he first started dialysis treatments, Fresenius Kidney Care clinic in Missoula charged $13,867.74 per session, or about 59 times the $235 Medicare pays for a dialysis session.
Tommy Martino/Kaiser Health News
hide caption
toggle caption
Tommy Martino/Kaiser Health News
Fresenius, one of the two largest dialysis providers in the U.S., has agreed to waive a $524,600.17 bill for a man who received 14 weeks of dialysis at a clinic in Montana.
NPR, Kaiser Health News, and CBS This Morning told Sovereign Valentine’s story this week, as part of the “Bill of the Month” series, a crowdsourced investigation that seeks to understand the exorbitant health care bills faced by ordinary Americans.
On Thursday, a representative from Fresenius told Sovereign’s wife, Dr. Jessica Valentine, that the company would waive their unpaid bill. Instead, they will be treated as in-network patients, and Fresenius will seek to negotiate with their insurer a rate higher than what the insurer has already paid. The Valentines are responsible only for their $5,000 deductible, which Sovereign, who goes by “Sov,” has already hit for the year. That leaves them with $0 left to pay on their in-network deductible.
“It’s a huge relief,” Sov said. “It allows me to put more energy back into just taking care of my health and not having stress hormones raging.” Sov said he hopes his experience will shed light on the problem of balance billing and help other patients in similar situations.
A 50-year-old personal trainer, Sov was diagnosed with kidney failure in January and sent for dialysis at a Fresenius clinic 70 miles from his home in rural Plains, Mont. A few days later, Sov and Jessica learned that the clinic was out-of-network and that they would be required to pay whatever their insurer didn’t cover.
The Valentines initially could not find an in-network option, and Sov needed dialysis three times a week to survive. After he underwent 14 weeks of dialysis with Fresenius, the couple received a bill for $540,841.90. Their insurer, Allegiance, paid $16,241.73, about twice what Medicare would have paid. Fresenius billed the couple the unpaid balance of $524,600.17 — an amount that is more than the typical cost of a kidney transplant.
Fresenius charged the Valentines $13,867.74 per dialysis session, or about 59 times the $235 Medicare pays for a dialysis session.
Fresenius spokesman Brad Puffer said that the Valentines should always have been treated as in-network patients because their insurer, Allegiance, is a subsidiary of Cigna, which has a contract with the dialysis company. Under this contract, Fresenius would have been paid a higher rate than what Allegiance paid. The Valentines, he said, were caught in the middle of a contract dispute between the companies.
“In the future, we pledge to better identify situations where we believe the insurer has incorrectly classified one of our facilities as being out of network,” Puffer said in a statement. “This will allow us to address the matter directly with the insurer in the first instance, without them placing the patient in the middle.”
Allegiance declined to comment for this story. Jessica Valentine questioned whether they may owe an out-of-network deductible and is waiting to hear what her insurer says about that.
Like her husband, Jessica is relieved that their bill seems to be resolved but worried that other people with bills like theirs might not be so lucky. She’s also grateful for all the attention their story has garnered. Montana Sen. Jon Tester’s office and their hospital’s insurance broker both offered to advocate for them. “And a nephrologist from Pennsylvania called me at work and expressed outrage and said she forwarded on our story to the medical director of Fresenius on our behalf,” Jessica wrote in an email.
Now that his bill has been resolved, Sov said he’ll be focusing on the next step in battling his kidney disease: a transplant. “I can just save my energy for that,” he said.
Bill of the Month is a crowdsourced investigation by NPR and Kaiser Health News that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it!
NPR’s Mary Louise Kelly speaks with lawyer Mike Moore, who is representing several states, counties and cities that are suing opioid manufacturers.
MARY LOUISE KELLY, HOST:
Litigation over the opioid crisis is heating up. A verdict in the first state case, Oklahoma, is expected next month. Meanwhile, in Ohio, a federal judge is overseeing litigation brought by more than 2,000 local governments – states, towns, counties – across the country.
Well, we’re going to spend these next few minutes with a man who has worked to convince all those governments to sue and who is working now to coordinate their efforts. A recent profile on “60 Minutes” called Mike Moore the unofficial commanding officer of opioid litigation in the U.S. And if his name sounds familiar, might be because he played a similar role two decades ago when he persuaded states to take on big tobacco.
Mike Moore, welcome back to ALL THINGS CONSIDERED.
MIKE MOORE: Thank you, Mary Louise. Glad to be here.
KELLY: So you represent several of the states that are suing – Arkansas, Louisiana, Mississippi, Ohio – also, several of the counties and cities who are litigating. And I wonder – how hard has it been to get all of your different clients, which must have different laws, different aims – how hard has it been to get them all on the same page?
MOORE: Well, it’s taken a long time. The defendants in these cases, as you might imagine, are not anxious to go to trial. With the revelation of where all the pills went, you know, that’s been in the newspaper and TV recently, there’s really nowhere for them to hide. We know what the story is. We know who’s at fault. So it’s really time for folks to focus on the public health crisis and come together and solve the problem. I mean, litigation is great. But it really is, you know, a tool that is used to try to get the truth out and to try to hold people accountable.
KELLY: You said we know who’s at fault.
MOORE: Sure.
KELLY: But when I last interviewed you a couple of years ago, in 2017, you acknowledge there is plenty of blame to go around in the opioid crisis, from doctors who overprescribed to pharmacists who filled out all those prescriptions to the government that failed to regulate and so on. Just make the case as simply as you can, why should the drug companies – manufacturers and distributors – be the ones held accountable above all those other parties?
MOORE: Well, first off, because the manufacturers are the ones who made the most money…
KELLY: And presumably, who can also pay out in a big settlement.
MOORE: Yeah, billions of dollars. And truthfully, the manufacturers probably made less money than the distributors. The distributors really made a mother lode of money. And then the Walgreens, CVSes, Walmarts, Ride Aides – they made a lot of money, too, dispensing these drugs and didn’t take the steps that they should have. The Controlled Substance Act is there for a reason. These are controlled substances. And frankly, everybody failed to control the flow of these drugs.
KELLY: Yeah. I mean, these companies, as you know – to sum up their defense in a line is that these were controlled substances. These were legal substances sold to legit patients who had prescriptions.
MOORE: They are. But in our country, the law pretty much says you have to tell the truth. And it’s clear that Purdue Pharma and the other companies – Johnson & Johnson and others – they didn’t tell the truth about the addictive nature of these drugs or what they should be used for. You know, they’re fine for long-term cancer pain and those type things. But you’re not supposed to get a 60-day supply for a tooth extraction and the like. And that’s what they kind of marketed these things for.
KELLY: How big a payout are you looking for to count as a success?
MOORE: You know, I think a better way to say it is – what does it take to start saving lives? You know, how do we get naloxone, you know, the antidote for overdoses, out to everybody that needs it? How do we get buprenorphine and treatment drugs out? How do we get a prevention education program out there to try to reverse the negative statements that were made by these companies years ago?
KELLY: All right. What’s that number?
MOORE: Well, that number is going to be in the multi-multi-multibillions of dollars. But we need to do it now. We don’t need to do it five years from now.
KELLY: Are the pockets of the opioid manufacturers being targeted in these suits deep enough to make that kind of payout? My impression is they’re – they don’t have as much money as, say, big tobacco manufacturers who you were suing back in the ’90s.
MOORE: Yeah, Purdue Pharma is close to bankruptcy, probably rightfully so. Their OxyContin sales are way down. Sacklers have some money that can be retrieved. Johnson & Johnson is a huge pocket. Then the distributors are big pocketbooks. The Walgreens, the CVS are big pocketbooks, and they all have some responsibility.
KELLY: What about your personal goal out of all this, Mike Moore? And I ask because when you and I spoke before, you talked about how this feels personal to you – that members of your family have overdosed, friends of yours have overdosed.
MOORE: Yep. For me, I really want to do something that makes a difference in saving people’s lives.
KELLY: You also said that whatever money might flow to you, you would be would be happy to donate in the…
MOORE: Absolutely.
KELLY: …Service of public health. Is that still where you stand?
MOORE: Absolutely. You know, I’m doing this for one reason. I don’t need to do this anymore. And I’m trying to make this a public crisis rather than just a big lawsuit. This isn’t a lawsuit. This is something to try, frankly, to solve a public health epidemic.
KELLY: Lawyer Mike Moore talking there about the efforts, which he is leading, to hold prescription drugmakers and distributors accountable in court for the opioid epidemic.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Allergen has announced a global recall of textured breast implants that are linked to a rare type of cancer, at the request of the Food and Drug Administration.
“Biocell saline-filled and silicone-filled textured breast implants and tissue expanders will no longer be distributed or sold in any market where they are currently available,” according to a company statement Wednesday.
The FDA said in a statement that while the overall incidence of the cancer appears to be low, it asked Allergan to initiate the Biocell implant recall “once the evidence indicated that a specific manufacturer’s product appeared to be directly linked to significant patient harm, including death.”
The agency does not recommend that people who already have the textured implants get them removed unless there are symptoms or problems, but it is providing information for patients and providers to consider.
The FDA said it requested the recall after a “significant increase” in cases of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), a type of non-Hodgkin lymphoma. Since its previous report in February, there have been 116 new cases and 24 deaths.
“Based on new data, our team concluded that action is necessary at this time to protect the public health,” said FDA Principal Deputy Commissioner Amy Abernethy.
Overall, according to the FDA, there have been 573 cases of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) and 33 patient deaths worldwide. The agency said 481 of the cases are attributed to the Allergan implants, and that among the deaths “12 of the 13 patients for which the manufacturer of the implant is known, are confirmed to have an Allergan breast implant at the time of their BIA-ALCL diagnosis.”
Based on the latest data, the FDA said, “our analysis demonstrates that the risk of BIA-ALCL with Allergan BIOCELL textured implants is approximately six times the risk of BIA-ALCL with textured implants from other manufacturers marketing in the U.S.”
The FDA first reported on a possible connection between implants and the rare cancer back in 2011, and Abernathy said the agency has continued to monitor reports in databases and patient registries and scientific studies pointing to risks.
Nearly 314,000 people received breast implants in the U.S. in 2018, according to the American Society of Plastic Surgeons. The group’s report does not distinguish between textured implants and other kinds.
“In the United States, the use of textured implants is much less common than the use of textured implants in Europe and Asia,” said plastic surgeon Daniel Maman, who is in private practice in New York and an assistant professor at Mount Sinai.
It’s not clear whether the texturing is actually responsible for the cancer or is just associated with a higher incidence of the disease. But Maman and others say the surface can interact with the surrounding scar tissue that the body forms as an immune response to the implant.
“It’s that response that is believed to cause the formation of the lymphoma,” Maman said, noting that he only uses smooth, round implants. Given the risks linked to textured implants, he said, “taking them off the market is very prudent and the right approach.”
The FDA’s action Wednesday is a change in course from a few months ago when advisers concluded there was a lack of scientific certainty about the health risks that breast implants pose to the millions of women who have them.
At the time, as NPR’s Patti Neighmond reported, “most members of the panel said there’s not enough evidence yet to rush textured implants off the market and that larger, longer-term studies are needed.”
Allergan said Wednesday that healthcare providers should no longer implant the Biocell implants and tissue expanders and that unused products should be sent back to the company. It said it would also work with customers about how to return unused products.
Different parts of the brain aren’t always in the same stage of sleep at the same time, notes neurologist and author Guy Leschziner. When this happens, an individual might order a pizza or go out for a drive — while technically still being fast asleep.
Frederic Cirou/PhotoAlto/Getty Images
hide caption
toggle caption
Frederic Cirou/PhotoAlto/Getty Images
We tend to think of being asleep or awake as an either-or prospect: If you’re not asleep, then you must be awake. But sleep disorder specialist and neurologist Guy Leschziner says it’s not that simple.
“If one looks at the brain during sleep, we now know that actuallysleep is not a static state,” Leschziner says. “There are a number of different brain states that occur while we sleep.”
As head of the sleep disorders center at Guy’s Hospital in London, Leschziner has treated patients with a host of nocturnal problems, including insomnia, night terrors, narcolepsy, sleep walking, sleep eating and sexsomnia, a condition in which a person pursues sexual acts while asleep. He writes about his experiences in his book The Nocturnal Brain.
Leschziner notes that the different parts of the brain aren’t always in the same stage of sleep at the same time. When this happens, an individual might order a pizza or go out for a drive — while technically still being fast asleep.
“Sometimes these conditions sound very funny,” Leschziner says. “But on other occasions they can be really life changing, resulting in major injury or, as one of the cases that I described in the book, in a criminal conviction.”
Interview highlights
On what we know about recall after a sleepwalking episode
We used to think that people don’t really remember anything that occurs in this stage. That seems to relate to the fact that the brain in parts is in very deep sleep whilst in other parts is awake. What we have learned over the last few years is that actually quite a lot of people have some sort of limited recall. They don’t necessarily remember the details of all the events or indeed the entirety of the event, but sometimes they do experience little snippets. … On one occasion, [a patient] dragged his girlfriend out of bed in the middle of the night because he thought that a tsunami was about to wash them away, and those kinds of events with strong emotional context are often better remembered.
On how sleepwalking demonstrates the brain can be in multiple sleep stages at once
Certain parts of the brain can remain in very deep sleep … [such as] the frontal lobes, which are the seats of our rational thinking or planning or restricting on normal behaviors, whereas other parts of the brain can exhibit electrical activity that is really akin to being wide awake. So, in particular, the parts of the brain that [can seem to remain awake] are [the ones] responsible for emotion, an area of the brain called the limbic system, obviously the parts of the brainthat are responsiblefor movement. And it’s this dissociation, this disconnect between the different parts of the brain in terms of the sleep stages, that actually give rise to these sorts of behaviors.
On what causes sleepwalking
We know that sleepwalkingand these related conditions seem to run very strongly in families. So there seems to be some sort of genetic predisposition to being able to enter into this disconnected brain state, and we know that anything that disrupts your sleep if you have that genetic predisposition can give rise to these behaviors. So, for example, I’ve seen people who have had non-REM parasomnia events [such as sleepwalking] triggered by the fact that they sleep in a creaky bed and their bed partner rolled over [or] sometimes a large truck [drove] past in the street outside the bedroom.
But there are also internal manifestations, internal processes that can give rise to these partial awakenings. So, for example, snoring or, more severe than snoring, sleep apnea, where people stop breathing in their sleep … anything that causes a change in the depth of sleep in people who are predisposed to this phenomenon of being in multiple sleep stages at the same time can give rise to these behaviors.
On sleep apnea
Sleep apnea describes the phenomenon of our airway collapsing down in sleep. … Our airway is essentially a floppy tube that has some rigidity, some structure to it as a result of multiple muscles. And as we drift off to sleep, those muscles lose some of their tension, and the airway becomes a little bit more floppy. Now when it’s a little bit floppy and it reverberates as we breathe in during sleep, that will result in snoring — the reverberation of the walls of the airway result in the noise.
But in certain individuals, the airway can become floppy enough or is narrow enough for it to collapse down and to block airflow as we’re sleeping. It’s normal for that to occur every once in a while for everybody, but if it occurs very frequently, then what happens is that sleep can be disrupted sometimes 10, sometimes 20, sometimes even 100 times an hour, because as we drift off to sleep, the airway collapses down, our oxygen levels drop, our heart rate increases, our brain wakes up again and our sleep is essentially being disrupted. …
We are now aware that obstructive sleep apnea has a range of long-term implications on our health in terms of high blood pressure, in terms of risk of cardiovascular disease, risk of stroke, impact on cognition and mental clarity. And there is now an emerging body of evidence to suggest that actually obstructive sleep apnea may be a factor in the development of conditions like dementia.
On the importance of having positive associations with your bed
If you’re a good sleeper, you tend to associate being in bedwith being in that place of comfort, that place where you go and you … feel cozy and you drift off to sleep and you wake up in the morning feeling wide awake and refreshed. But for people with insomnia, they often associate bed with great difficulty getting off to sleep, with the dread of the night ahead, with the fact that they know that when they wake up in the morning they will feel horribly unrefreshed and unrested. And so the environment that we normally would associate with sleep becomes an instrument of torture for them. And so a lot of the advances that have been made in this area about treating insomnia are really directed towards breaking down those negative associations that people have with their sleeping environment if they have insomnia and rebuilding positive associations. So trying to utilize the brain’s own mechanisms for drifting off to sleep and trying to reduce the anxiety surrounding sleep in order to reestablish a normal sleep pattern.
There has been a bit of a sea change in the last few years away from these drugs. We know that these drugs [are] sedatives. So the first thing to know is that they do not mimic normal sleep. They’re associated with some major problems. So some of these drugs are, for example, associated with an increased risk of road traffic accidents in the morning, because of a hangover effect. They’re associated with an increased risk of falls in the elderly, for example. And we know that people can develop a dependency on these drugs and can also habituate, by which I mean that they require ever-increasing doses to obtain the same effect.
In the long term, there are now some signals coming out of the work that is being done around the world that suggest that some of these drugs are actually associated with an increased risk of cognitive decline and dementia. And whilst that story is not completely understood — and it may be that people who have insomnia in themselves are predisposed to dementia or actually that insomnia may be a really early warning sign of dementia — [it] certainly gives us cause for concern that perhaps we shouldn’t be using these drugs quite as liberally as we have done historically. And so therefore the switch to behavioral approaches, approaches like cognitive behavioral therapy for insomnia, has been really driven by some of these concerns.
On his recommendation that you read before bed
Provided you are not reading on a tablet or a laptop, [and instead an] old-style analog book, I would highly recommend. It’s a good way of reducing your light exposure. Keeping your mind a little bit active so that you’re not concentrating on the prospect of having to drift off to sleep until you’re really tired. It’s a very good way of keeping your mind occupied.
Sam Briger and Mooj Zadie produced and edited the audio of this interview. Bridget Bentz and Molly Seavy-Nesper adapted it for the Web.
NPR’s Ari Shapiro speaks with Dr. Ranit Mishori, a family doctor, and a member of Physicians for Human Rights, about the job listing for a doctor to work at an ICE Processing Center.
ARI SHAPIRO, HOST:
Let’s talk about a job posting for a doctor to work at an immigrant detention facility in rural Louisiana. This opening has caught people’s attention for a few reasons. First of all, the job pays $400,000 for a doctor with just two years’ experience. And the company doing the hiring, GEO Group, wants someone who is, quote, “philosophically committed to the objectives of this facility.” The facility has a thousand beds for immigrant detainees.
Dr. Ranit Mishori noticed this listing on the Journal of the American Medical Association Career Center. She’s a professor of family medicine at Georgetown and a member of Physicians for Human Rights.
Welcome to the studio.
RANIT MISHORI: Thank you so much, Ari.
SHAPIRO: How unusual would it be for a doctor with two years’ experience to make $400,000 a year?
MISHORI: Well, it’s very unusual, especially for somebody who is a general practitioner. This is way more than I’m making, so the job really caught my attention for a variety of reasons.
SHAPIRO: And you’re living in D.C., a city with a cost of living much higher than rural Louisiana.
MISHORI: Exactly.
The other thing is they’re not asking for a board certification, which usually is a marker for competency of some sort.
SHAPIRO: Explain what a board certification represents.
MISHORI: Board certification are additional exams that people who graduate from residency programs have to take to show that they can deliver the best high-quality care. They’re not asking for that.
SHAPIRO: And then there’s that line – philosophically committed to the objectives of this facility. How do you interpret that?
MISHORI: Well, to me, when I read that ad after the initial surprise about the experience necessary and the salary, this was really very concerning – even chilling – to think about what I interpret to be a loyalty test. This, to me, was a very, very specific example of what we call in medical ethics dual loyalty.
SHAPIRO: Explain that concept of dual loyalty.
MISHORI: Dual loyalty is something that relates to the potential conflict between clinicians’ duties to their patients and their obligations to their employers. When these organizations have sometimes questionable tasks to fulfill, that becomes a very, very serious almost ethical minefield, I would say.
SHAPIRO: You and I have both been to immigration detention centers. What do you imagine the work will be like?
MISHORI: Well, I think when you talk about any correctional facility, especially immigration detention centers, there are a couple of hats that one has to wear. One is to take care of routine medical issues – so somebody has a headache, somebody has an infection, is vomiting. But also, we’re talking about people who are coming with immense trauma, people who may have injuries, people who have suffered from violence. You need to address that in some ways. There’s also making sure that there’s no spread of contagious diseases, that people are being nourished well. So it’s a very big job.
SHAPIRO: Isn’t it important to have the best medical personnel possible in those facilities? Wouldn’t you want somebody extremely qualified to be hired for a job like this?
MISHORI: Absolutely. You would want the most competent, the most compassionate physician that you can find. But those are not necessarily the physicians that they’re trying to hire based on the ad that I was looking at.
SHAPIRO: As you were talking about dual loyalty….
MISHORI: Yeah.
SHAPIRO: …Is there a specific example you can give us to help listeners understand how this plays out in the real world?
MISHORI: So it can start from you being a sports physician, and your star forward is injured, but you want to get her back in play because you want the team to win. So that’s one end. But it goes all the way to facilities where you are withholding treatment as a means of punishment, to giving people medications against their consent and without giving them the right to refuse.
SHAPIRO: We heard some of this at Guantanamo Bay, for example.
MISHORI: Exactly. So Guantanamo Bay is a really good example – also, force-feeding of hunger strikers.
SHAPIRO: And I guess the point is that while there may be black-and-white scenarios, there are a whole lot of gray scenarios, too. And when you’re in the middle of one, it can be hard to tell.
MISHORI: Right. And one of the grayest scenarios is you’re in a facility where you are the doctor. The person comes in for a headache, and you notice that they have scars on their back from being beaten. And you’re not doing anything. You’re not asking questions about it. You’re not documenting it in a chart, or you’re not reporting it to anybody. One of the things we try to teach in medicine is, really, the foundational idea that we need to always act in the best interest of the patient. And oftentimes, these scenarios do not lend themselves to doing that.
SHAPIRO: You can’t just keep your blinders on is what you’re saying.
MISHORI: You should not. People do, but you shouldn’t.
SHAPIRO: Dr. Ranit Mishori, thank you very much.
MISHORI: Thank you.
SHAPIRO: She’s a family physician and member of Physicians for Human Rights. We also asked GEO Group for comment about the amount of experience required and the philosophical commitment noted in the job listing. A spokesperson did not answer those questions but wrote in a statement, in part, (reading) we are deeply committed to delivering high-quality, culturally responsive services in safe and humane environments.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Clare Coleman, CEO of the National Family Planning and Reproductive Health Association, talks with NPR’s Sarah McCammon about recent changes to Title X regulations.
SARAH MCCAMMON, HOST:
Family planning clinics around the country that provide health services to low-income Americans have been getting some mixed messages recently from the federal government. This past week, the Trump administration said it would immediately begin enforcing new rules for the Title X family planning program, which would eliminate funding to organizations that provide or counsel patients about abortion. Then this weekend, we learned that Trump administration officials are now saying they will not immediately take action against groups deemed to be working in good faith to comply.
Clare Coleman is the CEO of the National Family Planning and Reproductive Health Association, which represents family planning clinics around the country. She joins us now.
Welcome.
CLARE COLEMAN: Thank you. It’s nice to be here.
MCCAMMON: So first, let’s talk about Title X. What is its role in providing reproductive health services, and how is the Trump administration trying to change the program?
COLEMAN: Well, the Title X program is now in its 49th year, and it was established to equalize access to modern forms of contraception and to help people both achieve pregnancy and prevent pregnancy. Last year, the Trump administration introduced a new set of rules, which represent the most consequential changes to the Title X program since it was enacted in 1970.
It changes the rules around how we can speak to patients about their contraceptive care. It allows providers to select the range of contraceptive methods that are offered and would allow providers to exclude methods that they object to, even if patients are interested in those methods. And it also limits the conversation that clinicians can have with patients once they have a positive pregnancy test.
MCCAMMON: Now, President Trump and other Republicans have run on promises to, quote, unquote, “defund Planned Parenthood.” This policy change is an effort to move in that direction, not just for Planned Parenthood but for other groups, of course. Now, the objection – I covered this issue quite a bit, and the objection from anti-abortion rights groups is that they say that funding for abortion should in no way be commingled or overlapping with other services. And so I would ask, why couldn’t these groups just stop providing abortions or referring patients for abortion?
COLEMAN: Well, the Title X program has prohibited use of Title X dollars for abortion care since its inception, and current grantees and some recipients follow very detailed rules that help you demonstrate when you have Title X funds that support family planning services, STI treatment and screening, cancer screening and then any abortion care that is provided in the same organization. Those rules go down to the very detail of financial reporting, and our grantees report quarterly. The administration has not been able to document either in the rule, in testimony before Congress or in any public documentation that there is any abuse whatsoever of the prohibition on Title X funds.
MCCAMMON: And what does this mean for the patients?
COLEMAN: It can be very confusing. And, candidly, it may be invisible. But I think for many low-income people, they know exactly how much cash they have in the bank, but they’re not necessarily tracking the rules. And one of our great fears is that folks are going to begin to encounter this when a service that used to be available to them is suddenly not available, or they’re presented suddenly with a bill.
So I’m concerned, and I think lots of us are concerned that all the decisions and considerations and guidance and coming back and forth between the feds and additionally the litigation that continues that patients won’t really begin to feel the impact until they ask for something that is no longer available to them where they live.
MCCAMMON: Clare Coleman is the CEO of the National Family Planning and Reproductive Health Association.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
NPR’s Sarah McCammon talks to Pamela Maraldo, former CEO of Planned Parenthood. She left the organization under similar circumstances as Dr. Leana Wen, who was ousted from her position this week.
SARAH MCCAMMON, HOST:
In July of 1995, the opening paragraph of a New York Times article read, quote, “at a time when both abortion rights and federal financing of family planning are under attack in Congress, Planned Parenthood, which has long led the fight for both, is in upheaval.” That story marked the departure of Planned Parenthood’s leader at the time, a woman with a medical background whose philosophy ran afoul of the organization then.
If that sounds familiar, it may be because this week, Planned Parenthood announced the departure of its most recent president, Dr. Leana Wen. Wen has said she was forced out over philosophical differences with the organization, including her desire to expand Planned Parenthood’s focus to a broader array of health issues. Almost exactly 24 years ago, Pamela Maraldo resigned over her own differences with Planned Parenthood. She has a Ph.D. in nursing, and she’s now CEO of the nonprofit group Girls Inc. Of New York City. Maraldo joins us now from our New York bureau.
Hello.
PAMELA MARALDO: Hello.
MCCAMMON: Now, the New York Times report that described your resignation in 1995 said that sources at the time said you had aroused opposition with your, quote, “emphasis on reshaping Planned Parenthood into a broad health organization that could compete in the era of managed care” – a focus that some of the group’s affiliates felt would inevitably diminish their role as advocates for abortion rights and low-income women’s access to health care.
Now, this week, in a letter explaining her ouster from Planned Parenthood, Dr. Leana Wen said she had come to the organization to work on a broad range of health care issues but that, quote, “the new board leadership has determined that the priority of Planned Parenthood moving forward is to double down on abortion rights advocacy.” She’s also said in an op-ed for The New York Times that she wanted to depoliticize abortion but that her approach seemed at odds with the direction the board wanted to go. What does this say about the trajectory of not just Planned Parenthood but also the abortion rights movement?
MARALDO: Certainly everybody would agree that reproductive rights are hanging the balance right now. It’s a tough time, and there are two schools of thought. I think that the leadership at Planned Parenthood has to do what it thinks is right. I don’t think there’s a right or wrong. For my part, I would do what I did, you know, last time around.
I think that when you look at the number of young people and poor women in the country that don’t have adequate health care, and you look at not the polarity in the debate but what women need on a day-to-day basis, it’s really rare that poor women have just one problem. It’s always accompanied by depression or hypertension or diabetes. So a public health physician who is a commissioner of health like Dr. Wen is going to see the world through that lens. I mean, she took an oath to do that. And similarly for a nurse, someone like me, you see the world in terms of health care delivery.
I think there is an argument to be made that the president of Planned Parenthood has to be strong in the advocacy arena right now when the media is so ever-present in all of our social issues – and certainly abortion’s at the top of that list. I think you have to be a strong advocate for reproductive rights, there’s no question about it – reproductive control and privacy, as Justice Ginsburg recently said. So we have to speak up and make sure that line in the sand is maintained, especially now with the Supreme Court having the constitution it has.
On the other hand, you could argue that, strategically, moving in the direction of broader health care will mitigate against, will, you know, help fight that fight in a much more integrated way, in a way that’s much more – that the American people would be receptive to.
MCCAMMON: And you talk about these two schools of thought, about how political to be versus how focused on health care, at least in terms of messaging. Is that a split that’s always been there within Planned Parenthood? Or is it just an old issue that was kind of dormant and has resurfaced, do you think?
MARALDO: I would say that your quote in the beginning was accurate. It’s resurfaced because I think they hired a physician. But it’s always dormant. And the fact is, their instincts were right, I believe, to hire a physician, a public health physician, because at the end of the day, if it weren’t a health care delivery network, they would be NARAL. And there is a great deal of credibility because Planned Parenthood does deliver other health services and an array of health services like, you know, prenatal care and pap tests and breast cancer screening and immunizations. Planned Parenthood has always provided a wide array of health care services. And so they can’t be de-emphasized It’s got to be based on women’s health and what they need.
MCCAMMON: You reference NARAL, of course, which is an abortion rights advocacy organization.
MARALDO: Right.
MCCAMMON: How do you think the mission of Planned Parenthood is and should be different from a group like NARAL and some of the others that do similar work?
MARALDO: I think that’s the point. Planned Parenthood delivers a wide array of services. And I think that – not that they don’t want to be good, strong voices and advocates for reproductive rights. I think, though, that there’s got to be a parallel concern about the health care of women in general and the services they deliver. So I had women come up to me and say, you’re so concerned about whether I’m going to have another baby or not. Why don’t you be more concerned about my prenatal care or the adequate, you know, nutrition? And I say, as a matter of fact, I am, and we are.
MCCAMMON: Dr. Wen’s departure after less than a year at Planned Parenthood came in a week when the Trump administration said it would start enforcing federal family planning rules that in effect cut a substantial amount of funding to Planned Parenthood.
MARALDO: Right.
MCCAMMON: You know, given that kind of landscape, how much of a role should the organization play, though, in lobbying against these kinds of policies that directly affect their health care mission?
MARALDO: Well, that’s what’s tricky. And that, they really do have to speak up now. Those voices need to be heard. They need a strong, vocal leader in support of reproductive rights, in support of family planning funds, in support of Medicaid funding for abortion. You know, poor women have, you know, two, three times the number of abortions, and they’re not provided for. So I think right now, times are critical, and we do need a strong voice of Planned Parenthood.
I’m not sure that Dr. Wen couldn’t have been that. I’m sure she understood that there – I don’t know this for a fact, but I can’t imagine that she was hired and knew the organization and didn’t understand that there was a strong role for – to speak up in the – in advocacy forums all over the country.
MCCAMMON: At the time when you were serving as CEO of Planned Parenthood in the early Clinton years, many Democrats were aligned with President Clinton, who famously said, abortion should be safe, legal and rare. As these issues continue to be debated in the public sphere, would you like to see a return by Planned Parenthood and other advocates to that kind of framing of this issue?
MARALDO: Yes, Sarah, I would – and reason being that I think with any medical procedure, any surgical procedure, the watchword should be prevention. I think the best practice is to try and prevent the thing in the first place. So I agree. I think that people that are pro-choice are afraid of stigmatizing abortion when they say it should be rare. And that’s not where I’m coming from. I’m coming from a place that too many trips to the doctor’s, medical procedures, surgical procedures, could be and should be prevented.
MCCAMMON: That was Pamela Maraldo, CEO of Girls Inc. of New York City. She was also a former president of Planned Parenthood back in the early 1990s.
Thank you so much.
MARALDO: Thank you, too, Sarah.
MCCAMMON: And we invited Planned Parenthood’s interim president, Alexis McGill Johnson, to appear on this program. We’re told she’s not available this weekend, but we are hoping to talk with her in the coming days.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.