
In The Fight For Money For The Opioid Crisis, Will The Youngest Victims Be Left Out?
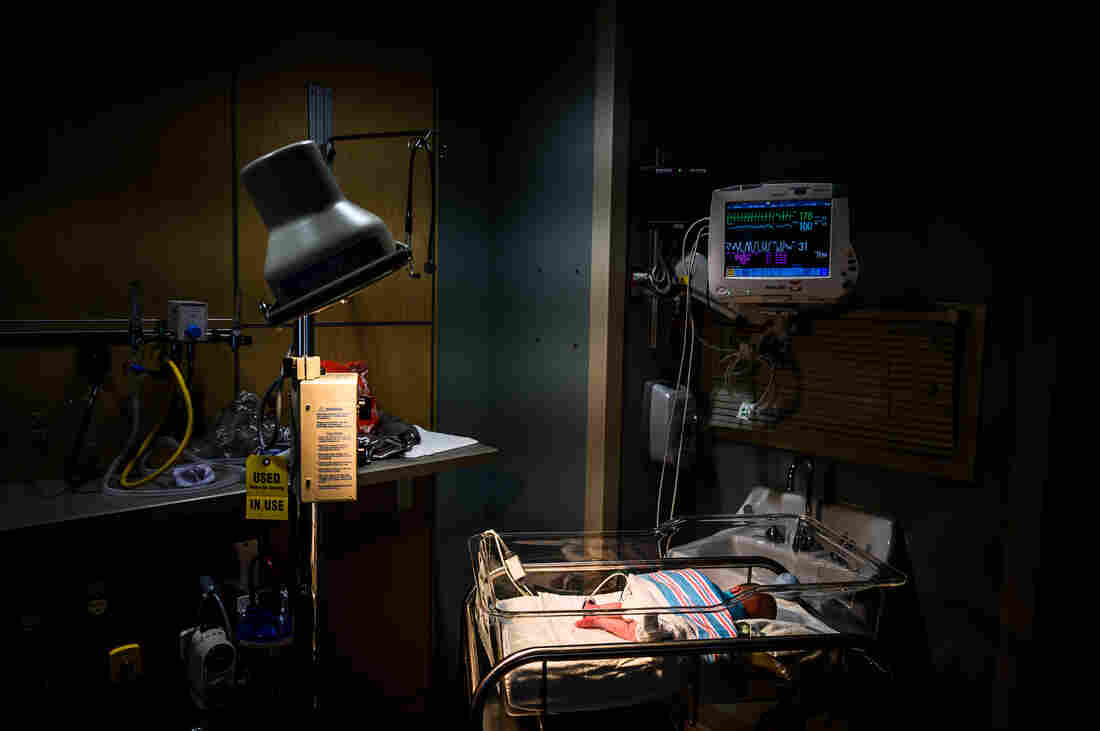
An infant is monitored for opioid withdrawal in a neonatal intensive care unit at the CAMC Women and Children’s Hospital in Charleston, W.Va., in June. Infants exposed to opioids in utero often experience symptoms of withdrawal.
Salwan Georges/The Washington Post/Getty Images
hide caption
toggle caption
Salwan Georges/The Washington Post/Getty Images
Babies born to mothers who used opioids during pregnancy represent one of the most distressing legacies of an opioid epidemic that has claimed almost 400,000 lives and ravaged communities.
In fact, many of the ongoing lawsuits filed against drug companies make reference to these babies, fighting through withdrawal in hospital nurseries.
The cluster of symptoms they experience, which include tremors, seizures and respiratory distress, is known as neonatal abstinence syndrome. Until recently, doctors rarely looked for the condition. Then case numbers quadrupled over a decade. Hospital care for newborns with NAS has cost Medicaid billions of dollars.
Studies indicate more than 30,000 babies with the condition are born every year in the U.S. — about one every 15 minutes. Although their plight is mentioned in opioid-related litigation, there are growing concerns that those same children will be left out of financial settlements being negotiated right now.

Robbie Nicholson now works as a mentor with a company called 180 Health Partners that helps women with addiction go through pregnancy. Her own newborn went through drug withdrawals, related to the medications she took to control her opioid cravings. She says most women she works with need a stable place to live and reliable transportation.
Blake Farmer
hide caption
toggle caption
Blake Farmer
Robbie Nicholson, a mother in Eagleville, Tenn., tried to comfort her second child while the baby slowly underwent withdrawal from drugs Nicholson had taken during pregnancy.
“The whole experience is just traumatizing, really,” Nicholson says.
Nicholson’s ordeal actually began right after her first pregnancy. To help with postpartum recovery, her doctor prescribed her a pile of Percocets. That was the norm.
“Back then, it was like I was on them for a full month. And then he was like, ‘OK, you’re done.’ And I was like, ‘Oh my God, I’ve got a newborn, first-time mom, no energy, no sleep, like that was getting me through,’ ” she says. “It just built and built and built off that.”
After developing a full-blown addiction to painkillers, Nicholson eventually found her way into recovery. In accordance with evidence-based guidelines, she took buprenorphine, a medication that helps keep her opioid cravings at bay. And then came another pregnancy.
But buprenorphine — as well as methadone, another drug used in medication-assisted addiction treatment — is a special kind of opioid. Its use during pregnancy can still result in withdrawal symptoms for the newborn, although increasingly physicians have decided that the benefits of keeping a mother on the medication, to help her stay sober and stable during pregnancy, outweigh the risk of her giving birth to a baby with neonatal abstinence syndrome.
Treatment protocols for NAS vary from hospital to hospital, but over time doctors and neonatal nurses have become better at diagnosing the condition and weaning newborns safely. Sometimes the mom and her baby can even stay together if the infant doesn’t have to be sent to the neonatal intensive care unit.
But not much is known about the long-term effects of NAS, and parents and medical professionals both worry about the future of children exposed in utero to opioids.
“I wanted her to be perfect, and she is absolutely perfect,” Nicholson says. “But in the back of my mind, it’s always going to be there.”
There are thousands of children like Nicholson’s daughter entering the education system. Dr. Stephen Patrick, a neonatologist in Nashville, says schools and early childhood programs are on the front lines now.
“You hear teachers talking about infants with a development delay,” he says. “I just got an email this morning from somebody.”
Studies haven’t proven a direct link between in utero exposure to opioids and behavior problems in kids. And it’s challenging to untangle which problems might stem from the lingering effects of maternal drug use, as opposed to the impacts of growing up with a mother who struggles with addiction and perhaps unemployment and housing instability as well. But Patrick, who leads the Center for Child Health Policy at Vanderbilt University, says that is what his and others’ ongoing research wants to find out.
As states, cities, counties and even hospitals go after drug companies in court, Patrick fears these children will be left out. He points to public discussion of pending settlements and the settlement deals struck between pharmaceutical companies and the state of Oklahoma, which make little or no mention of children.
Settlement funds could be used to monitor the health of children who had NAS, to pay for treatment of any developmental problems, and to help schools serving those children, Patrick explains.
“We need to be in the mix right now, in schools, understanding how we can support teachers, how we can support students as they try to learn, even as we work out was there cause and effect of opioid use and developmental delays or issues in school,” he says.

New mothers in recovery for opioid addiction meet with a support group in Oak Ridge, Tenn. Most had newborns who endured drug withdrawals at birth, known as neonatal abstinence syndrome.
Blake Farmer
hide caption
toggle caption
Blake Farmer
But it’s a nuanced problem with no consensus on where money is most needed, even among those who have been working on the problem for years.
Justin Lanning started Nashville-based 180 Health Partners, which works with mothers at risk of delivering a baby dependent on opioids. Most are covered by Medicaid. And those Medicaid departments in each state pay for most of the NAS births in the U.S.
“We have a few departments in our country that can operate at an epidemic scale, and I think that’s where we have to focus our funds,” he says.
Lanning sees a need to extend government-funded insurance for new mothers, since in states like Tennessee that never expanded Medicaid, these moms can lose health coverage just two months after giving birth. That often derails the mother’s own drug treatment funded by Medicaid, he says.
“This consistency of care is so key to their recovery, to their productivity, to their thriving,” Lanning says of new mothers in recovery.
Nicholson now has a job at 180 Health Partners, assisting and mentoring pregnant women struggling with addiction. Nicholson says their biggest need is a stable place to live and reliable transportation.
“I just feel kind of hopeless,” she says. “I don’t know what to tell these women.”
There are many needs, Nicholson says, but no simple fix. Those who work with mothers in recovery fear any opioid settlement money may be spread so thin that it doesn’t benefit their children — the next generation of the crisis.
This story comes from NPR’s reporting partnership with Nashville Public Radio and Kaiser Health News.
They Bring Medical Care To The Homeless And Build Relationships To Save Lives

Licensed practical nurse Stephanie Dotson measures Kent Beasley’s blood pressure in downtown Atlanta in September. Dotson is a member of the Mercy Care team that works to bring medical care to Atlanta residents who are homeless.
Bita Honarvar for WABE
hide caption
toggle caption
Bita Honarvar for WABE
Herman Ware sits at a small, wobbly table inside a large van that’s been converted into a mobile health clinic. The van is parked on a trash-strewn, dead-end street in downtown Atlanta where homeless residents congregate.
Ware is here for a seasonal flu shot.
“It might sting,” he says, thinking back on past shots.
Ware grimaces slightly as the nurse injects his upper arm.
After filling out some paperwork, he climbs down the van’s steps and walks back to a nearby homeless encampment where he’s been living. The small cluster of tents sits below an interstate overpass, next to a busy rail line.
Ware hasn’t paid much attention to his medical needs lately, which is pretty common among people living on the street. For those trying to find a hot meal or a place to sleep, health care can take a backseat.
“Street medicine” programs, like the outfit giving Ware his flu shot, aim to change that. Mercy Care, a health care nonprofit in Atlanta, operates a number of clinics throughout the city that mainly treat poor residents, and also has been sending teams of doctors, nurses and other health care providers into the city’s streets since 2013. The idea is to treat homeless people where they live.

“When we’re coming out here to talk to people, we’re on their turf,” says nurse practitioner Joy Fernandez de Narayan (right) in Atlanta. She and licensed practical nurse Stephanie Dotson (left), say showing patients respect is important in every setting.
Bita Honarvar for WABE
hide caption
toggle caption
Bita Honarvar for WABE
This public health strategy can now be found in dozens of cities in the U.S. and around the world, according to the Street Medicine Institute, which works to spread the practice.
Building relationships to give care
Giving shots and conducting exams outside the walls of a health clinic comes with unique challenges.
“When we’re coming out here to talk to people, we’re on their turf,” says nurse practitioner Joy Fernandez de Narayan, who runs Mercy Care’s Street Medicine program.
A big challenge is getting patients to accept help, whether it comes in the form of a vaccination or something simpler — like a bottle of water.
“We’ll sit down next to someone, like ‘Hey, how’s the weather treating you?’ ” she says. “And then kind of work our way into, like, ‘Oh, you mentioned you had a history of high blood pressure. Do you mind if we check your blood pressure?’ “
The outreach workers spend a lot of time forging relationships with homeless clients, and it can take several encounters to gain someone’s trust and get them to accept medical care.

Dotson gives a flu shot to Sopain Lawson, who lives in a homeless encampment under a bridge in downtown Atlanta. It can take several encounters to gain someone’s trust and get them to accept medical care, the health team finds.
Bita Honarvar for WABE
hide caption
toggle caption
Bita Honarvar for WABE
Their persistent encouragement was helpful for Sopain Lawson, who caught a debilitating foot fungus while living in the encampment.
“I couldn’t walk,” Lawson says. “I had to stay off my feet. And the crew, they took good care of my foot. They got me back.”
“This is what street medicine is about — going out into these areas where people are not going to seek attention until it’s an emergency,” says Matthew Reed, who’s been doing social work with the team for two years.
“We’re trying to avoid emergencies, but we’re also trying to build relationships.”
“Go to the people”
The street medicine team uses the trust they’ve built with patients to eventually connect them to other services, such as mental health counseling or housing.
Access to those services may not be readily available for many reasons, says Dr. Stephen Hwang, who studies health care and homelessness at St. Michael’s Hospital in Toronto. Sometimes the obstacle — say, lacking enough money for a bus ticket — seems small, but is formidable.
“It may be difficult to get to a health care facility, and often there are challenges, especially in the U.S., where people don’t have health insurance,” Hwang adds.

Social worker Matthew Reed (right) talks with Lawson near her tent home in downtown Atlanta. Reed says,”This is what street medicine is about: going out into these areas where people are not going to seek attention until it’s an emergency.”
Bita Honarvar for WABE
hide caption
toggle caption
Bita Honarvar for WABE
Georgia is one of a handful of states that has not expanded Medicaid to all low-income adults, which means many of its poorest residents don’t have access to the government-sponsored health care program. But even if homeless people are able to get health coverage and make it to a hospital or clinic, they can run into other problems.
“There’s a lot of stigmatization of people who are experiencing homelessness,” Hwang says, “and so often these individuals will feel unwelcome when they do present to health care facilities.”
Street medicine programs are meant to break down those barriers, says Dr. Jim Withers. He’s medical director of the Street Medicine Institute and started making outreach visits to the homeless back in 1992, when he worked at a clinic in Pittsburgh.
“Health care likes people to come to it on its terms,” Withers says, while the central tenet of street medicine is, “Go to the people.”

Clinic patient Lawson (center) and nurse practitioner Fernandez de Narayan (right) share a hug outside the Mercy Care van, after the September check-in. “We’re trying to avoid emergencies, but we’re also trying to build relationships,” says social worker Reed (left).
Bita Honarvar for WABE
hide caption
toggle caption
Bita Honarvar for WABE
Help, with respect
Mercy Care in Atlanta spends about $900,000 a year on its street medicine program. In 2018, that sum paid for direct treatment for some 300 people, many of whom got services multiple times. Having clinics on the street can help relieve the care burden of nearby hospitals, which Withers says don’t have a great track record when it comes to treating the homeless.
“We’re not dealing with them well,” Withers admits, speaking on behalf of American health care in general. In traditional health settings, homeless patients do worse compared to other patients, he says. “They stay in the hospital longer. They have more complications.”
Those extra days and clinical complications mean additional costs for hospitals. One recent estimate cited in a legislative report on homelessness suggested that more than $60 million in medical costs for Atlanta’s homeless population were passed on to taxpayers.
Mercy Care says its program makes homeless people less likely to show up in local emergency rooms and healthier when they do — which saves money.
It’s past sundown when the street medicine team rolls up to their final stop: outside a church in Atlanta where homeless people often gather. A handful of people have settled down for the night on the sidewalk. Among them is Johnny Dunson, a frequent patient of the street medicine program.
Dunson says the Mercy Care staffers have a compassionate style that makes it easy to talk to them and ask for help.
“You gotta let someone know how you’re feeling,” Dunson says. “Understand me? Sometimes it can be like behavior, mental health. It’s not just me. It’s a lot of people that need some kind of assistance to do what you’re supposed to be doing, and they do a wonderful job.”
Along with the medical assistance, the staff at Mercy Care give every patient big doses of respect and dignity. When you’re living on the street, it can be hard to find either.
This story is part of NPR’s reporting partnership with WABE and Kaiser Health News.
Jake Burton Carpenter, The Godfather Of Snowboarding, Dies At 65

The man known as “The Godfather of Snowboarding” died Wednesday at the age of 65. Jake Burton Carpenter brought the sport to the masses, through the company he founded.
AILSA CHANG, HOST:
The man called the soul of snowboarding has died. Jake Burton Carpenter was the founder of the iconic Burton Snowboards company. And as Vermont Public Radio’s Liam Elder-Connors reports, he helped open up the ski slopes to a whole new crowd.
LIAM ELDER-CONNORS, BYLINE: Fischer Van Golden is working at a ski and snowboarding shop in South Burlington. The store is buzzing as customers look through the dozens of brightly colored snowboards leaning against the wall. Van Golden says the store is close to the main Burton headquarters, which means it sells a good amount of the company’s gear. He reaches over and takes a board down.
FISCHER VAN GOLDEN: So the Burton Custom is probably one of the most iconic snowboards in the whole sport. It’s the one board they always continue to have in their line.
ELDER-CONNORS: Van Golden says he’s been working in the snowboard industry for a while, and Burton products have been a big part of his life. Even as a kid, he used to eagerly wait each year for the new catalog of Burton products.
VAN GOLDEN: And then just, like, obsessing over all the different products that were in it and, like, memorizing everything.
ELDER-CONNORS: Burton Snowboards was founded by Jake Burton Carpenter in 1977. According to the company, Carpenter worked as a bartender by night. And during the day, he built snowboards in his Vermont barn and tested them on nearby hills. Carpenter didn’t invent the snowboard. A similar device, called the Snurfer – think snow surfer – was invented about 10 years before Carpenter started his company. But Van Golden says Carpenter revolutionized the design of snowboards.
VAN GOLDEN: He sort of pioneered the sport itself and came up with the idea of strapping your feet actually to the board rather than just, like, surfing on top of the board with no binding. He created, you know, bindings that attach you to the board so you can actually, like, carve and control the board much better.
ELDER-CONNORS: While Carpenter is widely credited with popularizing the sport, it wasn’t his first thought when he started the company. In a 2016 StoryCorps interview, Carpenter said at first he thought of the company as a get-rich-quick scheme.
(SOUNDBITE OF ARCHIVED RECORDING)
JAKE BURTON CARPENTER: It became much more than that because I didn’t get rich quick.
ELDER-CONNORS: Carpenter says his focus soon turned to nurturing the sport. In the early days of the company, many ski resorts didn’t even allow snowboarders on the mountains.
(SOUNDBITE OF ARCHIVED RECORDING)
BURTON CARPENTER: After a couple of years, it became much more important to me that I was right about the decision that there was a sport there. And I focused not about my own material needs or accomplishments or whatever; I just thought about the sport.
ELDER-CONNORS: Now, thanks in part to Carpenter’s work, when you go to the slopes, you can’t miss the groups of kids on snowboards who fly off big jumps, trying to land complicated tricks.
In a company-wide email this morning, Burton told its employees that Carpenter, the, quote, “soul of snowboarding,” died Wednesday night from complications due to cancer. And they urged their employees to honor Carpenter by going snowboarding.
For NPR News, I’m Liam Elder-Connors in Colchester, Vt.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
The Great Cranberry Crash Of 1959
How did the cranberry go from a seasonal, Thanksgiving favorite to an all-year round, ubiquitous supermarket staple?
ARI SHAPIRO, HOST:
This time next week, many of us will sit down to a plate of turkey, mashed potatoes, stuffing and cranberries. Sixty years ago, cranberries were missing from the Thanksgiving table. There was a scare over potentially cancerous cranberries. All sales stopped. The cranberry business nearly died. Stacey Vanek Smith and Adrian Ma from our daily economics podcast The Indicator From Planet Money have this report on the great cranberry crash of 1959.
STACEY VANEK SMITH, BYLINE: It was early November 1959 when Arthur Flemming got some distressing news. He was the secretary of Health, Education and Welfare under President Eisenhower, and he had just learned that samples of cranberries collected in Oregon and Washington contained traces of an herbicide called amino triazole.
ROBERT COX: Amino triazole was known to cause thyroid cancer in rats.
VANEK SMITH: This is Robert Cox, author of the book “Massachusetts Cranberry Culture.”
COX: Carcinogens had been banned for agricultural use the previous year – 1958. And so he said, we have a problem.
ADRIAN MA, BYLINE: The problem was Thanksgiving was less than three weeks away. And on top of turkey, millions of Americans would soon be eating cranberry sauce.
VANEK SMITH: So on November 9 almost exactly 60 years ago, Flemming issued a statement, warning the public of the contamination and the potential cancer risk. Within hours, grocery stores around the country pulled cranberry products from their shelves. As news about the contaminated cranberries swept the nation, the market for them basically ground to a halt.
JOHN DECAS: We had 40 trailer loads of cranberries canceled within one hour after that announcement.
VANEK SMITH: John Decas is co-owner of Decas Cranberry Products in Carver, Mass. At the time of the cranberry scare, he was in his mid-20s and had just started working in the family business.
MA: John says the rest of that year, they did not sell a single berry.
VANEK SMITH: Later, lab tests only found traces of amino triazole in about 1- or 2% of the fruit they inspected. And Congress would pay the growers about $8.5 million to compensate them for lost sales. Still, the damage was pretty much done.
MA: Part of what made the cranberry scare so hard on producers like John was the timing – just days before Thanksgiving. And back then, Thanksgiving was the cranberry industry.
VANEK SMITH: The cranberry industry had to figure out how to get people to eat cranberries not just on Thanksgiving.
MA: In the early 1960s, Ocean Spray had this idea. They thought, if we want people to consume more cranberries, we need to think beyond sauce. And so cranberries went from being a once-a-year fruit to something you could have in any season. Cranberries are now a global commodity. Last year, the U.S. exported almost half a billion dollars’ worth of cranberry products, and U.S. farmers produced almost 9 million barrels.
VANEK SMITH: After the scare of 1959, the cranberry industry came out on top.
MA: That is until last summer.
VANEK SMITH: Trade war.
MA: Trade war – what else? As part of its retaliation, China imposed a 25% tariff on dried cranberries. And soon, sales to China fell by nearly half. On top of that, cranberry growers are now facing a massive surplus. For years, the fruit’s popularity drove increased production in the U.S., Canada and Chile. And now there is a global glut of cranberries.
VANEK SMITH: So the industry is taking a page from the cranberry crisis playbook back from 1959. Companies are doubling down and trying to find a new hit product. The next cranberry juice cocktail or the next dried cranberry.
MA: Adrian Ma.
VANEK SMITH: Stacey Vanek Smith, NPR News.
(SOUNDBITE OF BLUE STATES SONG, “YOUR GIRL”)
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
UAW President Gary Jones Abruptly Resigns Amid Corruption Scandal

Former United Auto Workers President Gary Jones speaks during the opening of contract talks with Fiat Chrysler Automobiles in Auburn Hills, Mich., in July 2019. Jones resigned Wednesday.
Paul Sancya/AP
hide caption
toggle caption
Paul Sancya/AP
The president of the United Autoworkers Union, Gary Jones, abruptly resigned Wednesday just as union leaders announced they would expel him and another top UAW official in an unfolding corruption scandal.
In a related development, General Motors (GM) filed suit against rival Fiat Chrysler Automobiles (FCA) alleging that the company bribed UAW officials in order to get favorable labor contracts and disadvantage GM.
Michigan Radio’s Sarah Cwiek reported that the UAW’s International Executive Board unanimously voted to expel Jones.
“That kickstarted the process to remove Gary Jones and another UAW official, Director Vance Pearson.
“Both men have been implicated in a corruption scheme that involved misusing union funds for personal expenses, then covering it up.
“Both Jones and Pearson had already taken leaves of absence. Pearson already faces federal charges, while Jones has so far not been charged.”
An attorney for Jones, Bruce Maffeo of New York, told The Associated Press that union president decided to resign before learning of the board’s action.
Hours earlier, GM filed its federal racketeering lawsuit alleging that FCA bribed UAW officials in order to get contracts allowing the company to pay some newer employees less money — known as two-tier pay — resulting in lower labor costs.
“This lawsuit is intended to hold FCA accountable for the harm its actions have caused our company and to ensure a level playing field going forward,” Craig Glidden, GM Executive Vice President and General Counsel, said in a statement.
The lawsuit alleges that FCA corrupted bargaining agreements in 2009, 2011 and 2015.
FCA responded with a statement dismissing GM’s lawsuit as “this extraordinary attempt at distraction” with claims that “are nothing more than a meritless attempt to divert attention from that company’s own challenges.”
GM’s lawsuit alleges that FCA’s former CEO Sergio Marchionne authorized bribes of more than $1.5 million paid to UAW officials. Marchionne died in 2018.
It also alleges that Marchionne hoped to force higher labor costs onto GM in hopes of furthering a plan to induce the company to merge with FCA.
As Michigan Radio’s Tracy Samilton reports,
“GM’s lawsuit piggybacks on a federal investigation into UAW corruption that began several years ago – resulting in three Fiat Chrysler executives going to prison, along with six guilty pleas (so far) by union officials.
“Federal authorities says the executives were involved in a bribery scheme meant to keep union officials “fat, dumb and happy,” (quoting one of the convicted FCA executives, Alphons Iacobelli) during contract talks.
“GM says normally, the union’s pattern bargaining results in similar labor costs for all three Detroit automakers.”
In ‘Canyon Dreams,’ A Navajo Town Struggles To Survive In An Often Hostile World

College and professional sports have a way of dominating the national headlines. But in some parts of America, high school athletics have become local obsessions.
In Pennsylvania, fans flock to school wrestling matches, while in Texas, high school football teams routinely sell out some of the state’s biggest stadiums.
In many parts of the western U.S., though, it’s the game of “rez ball” that has sports fans enchanted. As Michael Powell writes in his wonderful new book, Canyon Dreams, rez ball — so named because it’s played on Native American reservations — is a unique spin on basketball, “a quicksilver, sneaker-squeaking game of run, pass, pass, cut, and shoot, of spinning layups and quick shots and running, endless running … Play was swift and unrelenting as a monsoon-fed stream.”
And not many teams play it better than the Wildcats of Chinle High School, located in the Navajo Nation in northeastern Arizona. Powell, a New York Times columnist, spent a season in the small town of Chinle, watching the Wildcats take to the hardwood, and spending time with those who call the reservation home. Canyon Dreams is the product of his time in and around Chinle, and it’s a remarkable achievement.
Powell focuses heavily Raul Mendoza, the school’s “respected, although perhaps not beloved” basketball coach, whose career leading teams in the Southwest spanned decades: “He had lived a dozen lives in seventy years of wandering.” Mendoza is an old-school coach who’s determined to take Chinle to the state championships; he loves telling “corny jokes and he could name no rapper, past, present, or future.”
At the beginning of the season, Mendoza’s Chinle team has the potential to be a powerhouse, though you wouldn’t know it to look at them: Only three of the players on his team are over 6 ft. tall; the Wildcats’ point guard, Josiah Tsosie, stands at 5 ft. 4 in. Still, they’re scrappers in the rez ball tradition, which puts a premium on pugnacity and physicality: “Custom dictated that players help their opponents to their feet. They as quickly knocked them down again.”
Many of Mendoza’s players aren’t quite sure what to make of their laconic, reserved coach; some resent him for leaving them on the bench, while others don’t appreciate his often caustic assessments of their on-court performance. Despite his hard edges, though, Mendoza clearly cares for his players, especially those who have had to endure difficulty:
“Mendoza harbored special affection for the lost. … To take a well-adjusted kid and train and mold him was rewarding; to break through to the desperate, to give hope where there was none, was another mission entirely.”
And none of the players on the team have had easy lives. Chinle, like many nearby towns, has been beset by poverty, unemployment, domestic violence and alcoholism: “I knew of no player on Mendoza’s team whose family had not lost a relative to the bottle and fetal alcohol syndrome deformed some infants,” Powell writes.
He spends time with a wide array of people who live on the reservation, and presents their stories with a sympathy that’s never condescending. The results of his interviews can be heartbreaking: At one point, he takes a walk with a Navajo jeweler who used to play rez ball as a teenager; the next day, Powell learns that the man passed out the night before, the result of drinking too much, and froze to death.
Canyon Dreams is a book about basketball the same way that Buzz Bissinger’s Friday Night Lights is a book about football — while sports are the ostensible focus, Powell’s real interest is the community that drives the team. That’s not to say Powell’s coverage of Chinle’s games isn’t fascinating; indeed, he recaps the matches with an expert pacing, and creates an atmosphere of suspense as the Wildcats’ season progresses. He’s an excellent sportswriter with an obvious love for the game, and he does a great job explaining what makes rez ball so unique.
But it’s his deep dives into the lives of those associated with Chinle and its high school that sets Canyon Dreams apart. He profiles not just the players and coaching staff, but also teachers, townspeople and activists, and the result is a moving portrait of what it’s like to live on the reservation. Powell even incorporates memoir into the book, writing about his own explorations of the town, and how he came to be so invested in its people.
Canyon Dreams is difficult to categorize, but it’s unmistakably beautiful. Powell is a gifted and giving writer, and his book is at once a reflection on youth and ambition and a fascinating chronicle of a town’s struggle to survive in a world that’s often cruel and hostile. “Nothing about a basketball season is easy,” as Mendoza says. “Neither is life.”
Snarky Puppy: Tiny Desk Concert

Credit: Emily Bogle/NPR
Seconds before we hit record, Snarky Puppy‘s bandleader, Michael League leaned in to ask if he could “do a little crowd work.” I suspect he waited until the last second on purpose, but it’s been easy to trust this band when they have an idea, judging by the three Grammy Awards they get to dust off at home after every tour run.
What resulted was a Tiny Desk first: League divided the audience into two sections, one side clapping out a 3/4 beat and the other half a 4/4 beat, creating a polyrhythm that I’m sure a handful of coworkers didn’t feel so confident trying to pull off. But this band pulls you in with simple instruction and a little faith.
Snarky Puppy has been a force for a while now, earning the ears of millions for more than a decade. And their secret sauce? A long-simmered recipe of jazz, funk and gospel. The band started as college friends in the jazz program at the University of North Texas back in 2003. But the formative era came a few years later, after League became a part of the gospel scene in Dallas and eventually brought the jazz students to church, where music plays a different role than it does in the classroom. In the pulpit, it’s a channel for spiritual healing, a communal experience between players and congregation. As an experiment, League pulled his jazz friends and his gospel bandmates into one ensemble, where the two groups bonded together and established ground-zero for building the sonic identity of Snarky Puppy.
Thirteen albums later, you can still hear these gospel and jazz orbits crashing into each other. They’re masters of theme and variation, offering anyone with a listening ear a place to grab hold. And people do. They’re a band whose lyric-less melodies are still yelled (sung back) to them at their concerts around the world, as a shared catharsis for everyone in the room.
SET LIST
- “Tarova”
- “Xavi”
MUSICIANS
Michael League: Bass; “JT” Thomas: drums; Nate Werth: percussion; Shaun Martin: keys; Bobby Sparks: keys; Justin Stanton: keys, trumpet; Jay Jennings: trumpet; Chris Bullock: saxophone, flute; Chris McQueen: guitar; Zach Brock: violin
CREDITS
Producers: Colin Marshall, Morgan Noelle Smith; Creative Director: Bob Boilen; Audio Engineer: Josh Rogosin; Videographers: Bronson Arcuri, Jack Corbett, CJ Riculan, Morgan Noelle Smith; Associate Producer: Bobby Carter Executive Producer: Lauren Onkey; VP, Programming: Anya Grundmann; Photo: Emily Bogle/NPR
America’s ‘Shame’: Medicaid Funding Slashed In U.S. Territories

Sandra King Young runs Medicaid in American Samoa, a U.S. territory that faces dramatic funding cuts to islanders’ health care unless Congress acts. “This is the United States’ shame in the islands,” she says.
Selena Simmons-Duffin/NPR
hide caption
toggle caption
Selena Simmons-Duffin/NPR
Right now, there are dozens of patients — U.S. citizens — in New Zealand hospitals who are fighting the clock. They have only a few weeks to recover and get home to the tiny island of American Samoa, a U.S. territory in the South Pacific.
“We have a cancer patient that is coming back in December,” says Sandra King Young, who runs the Medicaid program in American Samoa. “We can only give him six weeks of chemo, radiation and surgery. He has a good chance of survival if he has the full year of treatment, but not six weeks. The patient and family understand, and since they have no money, they have agreed to come back.”
The federal money to fully fund the Medicaid program in American Samoa and in all other U.S. territories is about to run out. As a consequence, the off-island referral program to treat conditions that the territory doesn’t have the local capacity or facilities to treat — the program that brought these patients to New Zealand — is getting shut down.
“It’s devastating for those people who need those lifesaving services,” King Young says. “People who need cancer treatment won’t get it. Children with rheumatic heart disease won’t get the heart surgeries that they need.”
All five of the U.S. territories affected — collectively home to more than 3 million Americans — are now desperately trying to figure out how to keep Medicaid running with only a fraction of the money they’ve had for the last several years. If Congress doesn’t increase the amount of designated money by the end of the year, the U.S. Virgin Islands and Guam say they would need to cut their Medicaid rolls in half; Puerto Rico says it would need to cut back dental and prescription drug services.
This is what people working on the issue have come to call the “Medicaid cliff.”
How did we get here?
When it comes to Medicaid, the federal government treats U.S. territories differently from how it treats states.
In U.S. states, the amount that the federal government contributes to Medicaid varies based on a formula in the law that relies on per capita income in each state. For instance, Alabama has a match rate of 72%; what this translates to is that for every dollar Alabama spends on Medicaid, the federal government contributes about $2.57 to the program.
But that’s not how it works in the territories, where even though the populations are all low income, the federal government’s match rate is set in statute at 55%. What this translates to is that for every dollar a U.S. territory spends on Medicaid, the federal government contributes $1.25.
The other significant difference is that the federal contribution to Medicaid in the territories is capped, with a set allotment of federal funds every year. Federal spending on Medicaid in states is not.
The low matching rate and the annual cap — that’s pretty much how it has always been for Medicaid in the territories, says Robin Rudowitz, who co-directs the Program on Medicaid and the Uninsured at the Kaiser Family Foundation. “These particular provisions historically have always been part of how they have been financed,” she says.
Here’s how the territories found themselves peering over the “Medicaid cliff.” For the last few years, the territories have had billions of dollars more in federal funding to run their programs than their usual capped allotments. First, the Affordable Care Act provided a one-time grant of $7.3 billion (which kicked off in 2011) for the territories’ Medicaid programs. Then, in 2017, after two Category 5 hurricanes ravaged Puerto Rico and the U.S. Virgin Islands, an extra $4.9 billion designated for their Medicaid programs was added to the 2018 Bipartisan Budget Act.

The Family Health Center Susana Centeno on remote Vieques island, part of Puerto Rico, was forced to close after it suffered damage from Hurricane Maria in 2017.
Xavier Garcia/Bloomberg/Getty Images
hide caption
toggle caption
Xavier Garcia/Bloomberg/Getty Images
Now, we’ve come to the cliff’s edge. Most of these two pots of money ran out at the end of September, with just a bit of funding from the ACA still available through the end of 2019.
That leaves, essentially, just the capped allotment of federal dollars for each of the territories — far less than what the territories have come to rely on to provide care to their Medicaid enrollees in recent years.
“The capped financing amounts were low and did not meet all of the needs of the population in the territories,” says Rudowitz. If the additional federal contributions are gone for good, she says, “given the share that they represent of the financing for Medicaid in these territories, it would mean major changes and reductions in care.”
The territories have known that this funding cliff was coming for years — the end to a major portion of the money was written into the ACA. Island health officials and care providers hoped Congress would have legislated a more permanent solution by now, but it hasn’t.
In recent months, Congress has passed continuing resolutions that have allowed the territories’ Medicaid programs to keep limping along. But without legislation that appropriates more money, the territories’ Medicaid programs all are in serious trouble.
The Medicaid and CHIP Payment and Access Commission, known as MACPAC, a nonpartisan government group that advises Congress on Medicaid policy, projected in July that all the territories will have budget shortfalls in 2020. When considered altogether, according to MACPAC’s report, their Medicaid programs will be more than $1 billion short.
This is why Medicaid directors in the U.S. territories are all sounding the alarm. King Young, of American Samoa, points to news coverage as far back as the 1960s that described her island as “America’s Shame in the South Seas” because of rampant pollution and neglect.
“Right now, this is the United States’ shame in the islands,” she says. “Tell me if that’s acceptable in the United States, to stand by and say, ‘Oh, sorry, we can’t give you that stent or that pacemaker, so it’s likely that you’ll have a stroke or heart attack and — that’s it.’ That’s what it means not to have enough Medicaid funding for the territories.”
“Full-court press” in Congress
The territories have been lobbying Congress, urging members to appropriate more funds for their Medicaid programs so health officials on the islands can avoid these hard choices — between, for instance, keeping a hospital going and paying for a patient’s cancer treatment.
Each territory has a nonvoting delegate in Congress. Puerto Rico also sent an additional delegation from the island last week to make the case to lawmakers that something must be done to stave off disaster.
“I would say that we’ve been doing a full-court press this entire calendar year,” says Jennifer Storipan, executive director of the Puerto Rico Federal Affairs Administration. “Gov. [Wanda] Vázquez has said that Medicaid funding is her highest priority for the island right now.”
A bill to temporarily increase funding to the territories’ Medicaid programs was passed by the House Energy and Commerce Committee in July but has yet to make it to the floor for a vote. It would greatly increase the federal match rate for Medicaid in all the territories and allocate a bonus $3 billion a year — but only for the next four years. There is no companion bill in the Senate.
“We’re in active negotiations with the Senate, but there is some opposition to our bill in the Senate,” says Rep. Darren Soto, D-Fla., who introduced the House legislation with Rep. Gus Bilirakis, R-Fla. Both represent districts in central Florida that have huge Puerto Rican populations, and Soto is of Puerto Rican descent. In the House, the bill has bipartisan support.
Opponents of the bill in the Senate say they worry that the billions of dollars that the territories are requesting could be misspent. Some senators have raised particular concerns about Puerto Rico. During a recent corruption probe, a Puerto Rican Medicaid official was arrested — that news emerged just a few days before a committee hearing on the territories’ Medicaid bill in July.
“So that didn’t help,” Soto says. Integrity provisions were added to the House bill, he says, specifically addressing concerns about Puerto Rico. “We do need to take it seriously and make sure that tax dollars are safeguarded,” he says, but adds, “There have been fraud instances in many states too, and we don’t take away their Medicaid funding.”
Some congressional Republicans note that the funding cliff was created by the Affordable Care Act, which gave extra funding to the territories for a limited time. In a letter to Secretary of Health and Human Services Alex Azar in July, several Republican members of the Senate Finance Committee raised concerns about Puerto Rico’s Medicaid spending.
“We are again confronting proposals for what amounts to another extension of boosted funding with no permanence or certainty and without any resolution of the Medicaid funding cliff constructed as part of the ACA,” they wrote.
“It is true: Giving these additional funds with a set expiration date, the legislation itself did create the cliff,” acknowledges the Kaiser Family Foundation’s Rudowitz. However, she says, Congress now should consider “the implications of letting that cliff happen and what that means to the health care systems in these territories.”
Planning for the worst
Medicaid program administrators from each of the territories gathered in an impromptu meeting outside the annual Medicaid directors conference last week. They have spent a lot of time together in Washington recently, testifying before congressional committees about the Medicaid funding crisis as it approaches.
“We were here in May. We were here in June,” Michal Rhymer-Browne, assistant commissioner with the Virgin Islands’ Department of Human Services, told NPR that day. “We pleaded. We shared ourselves — everything that we could.”
Despite their pleas, Congress has yet to act.
There are three options for managing a slashed budget for a program like Medicaid: reduce the size of payments to providers, cut the rolls or cover fewer services. All the territories say there’s no way to go lower on provider payments — Puerto Rico’s struggle with provider flight because of low pay is well known. So cutting the rolls and covered services is where the programs would need to find cuts, representatives of the territories say.
“Guam and [the Northern Mariana Islands] are about to topple over the cliff,” Rhymer-Browne says. “And for the Virgin Islands, we are nearing the cliff and seeing the bottom right now.”
Many of the territories would like to make improvements in the care they provide — invest in better facilities, recruit great health care providers, improve preventive care. All of that comes with upfront costs, they say, and they’ve had so much budget uncertainty that it has been impossible to move forward with those kinds of projects.
Right now, they’re just trying to keep the lights on.
“The urgency is here for us to let our congressional members know — even going to January is extremely dangerous,” Rhymer-Browne says. “It’s already catastrophic for our territories. We really need them to make a move.”
Gordon Sondland Was A Low-Profile Hotel Owner. Until He Went To Work For Trump

Hotel owner Gordon Sondland, who is scheduled to testify before Congress on Wednesday, is a pivotal witness in the impeachment inquiry.
Carlos Jasso/Reuters
hide caption
toggle caption
Carlos Jasso/Reuters
When Gordon Sondland arrived at the Capitol last month to provide what would be pivotal testimony in the Trump impeachment inquiry, a reporter asked the U.S. ambassador to the European Union, “Are you here to salvage your reputation?”
“I don’t have a reputation to salvage,” Sondland shot back.
Until recently, Sondland, 62, had a pretty low profile outside his hometown of Portland, Ore., where he and his wife, Katy Durant, are big Republican donors and contributors to numerous arts and civic organizations.
Now, as Sondland prepares to testify publicly before congressional investigators Wednesday, he finds himself in the middle of a Category 5 political storm.
Congressional investigators are looking into whether President Trump withheld security assistance from Ukraine to pressure the government to say it was investigating former Vice President Joe Biden’s son Hunter, who served on the board of a Ukrainian gas company.
Sondland, who helped reach out to the Ukrainian government on Trump’s behalf, first told Congress that the president was simply interested in battling corruption. He had demanded no favors in exchange for security assistance, he claimed.
But Sondland later amended his testimony, saying the aid package was in fact contingent on an investigation into the Bidens.
A strive for prominence
The impeachment inquiry has given Sondland a notoriety he never bargained for when he became EU ambassador.
The son of Holocaust survivors, Sondland dropped out of college early and got into commercial real estate. At just 28, he bought and renovated the bankrupt Roosevelt Hotel in Seattle, where he was born.
Today, his company, Provenance Hotels, owns 14 hotels, including six in Portland.
“He sees a good property that’s kind of in the right location and makes enough of an investment in it to make it a highly desirable place to stay,” says Len Bergstein, a public affairs consultant who has worked with Sondland.
Sondland has worked hard to be seen as a civic leader and cares a lot about how he is seen, Bergstein says. When Sondland worked out a deal with local government to acquire some land for a hotel, he insisted that he be referred to as a “pillar of the community” in the press release the city put out, Bergstein says.
“He was in many ways exercising his political muscles to try and up his profile, to take him from a kind of a noted and successful businessperson in a relatively narrow sense to much larger circles of prominence in the community,” Bergstein says.
According to Oregon Business, Sondland is a big fan of Ayn Rand, whose books promoting free market capitalism are popular with many libertarian conservatives.
But he has mainly donated to moderate Republicans like Jeb Bush and even a few Democrats, according to Sheila Krumholz, executive director of the Center for Responsive Politics.
A complicated relationship with Trump
His relationship with Trump is complicated. Sondland publicly broke with him following the then-presidential candidate’s attack on a Gold Star Muslim family. Yet Sondland also became a “bundler” for Trump, using his network of Portland political donors to help Trump get elected.
“In that election he gave nothing to Trump but he was listed as one of Trump’s bundlers in 2016, and of course being a bundler gives you more clout than just giving a single donation,” Krumholz says.
Sondland also donated $1 million to Trump’s inauguration through four companies Sondland controls.
A lot of people in liberal Portland have been taken aback by Sondland’s willingness to work in the Trump administration, Bergstein says.
“It was a surprise when Gordon found Donald Trump as an acceptable candidate. That wasn’t his type of Republican that he supported,” he says.
And Sondland has already paid a price for that support.
He is sometimes confronted by demonstrators when he goes out in public. And Democratic Rep. Earl Blumenauer, who represents the Portland area, has called for a boycott of his hotels.
Want New Taxes To Pay For Health Care? Lessons From The Affordable Care Act

A demonstrator celebrated outside the U.S. Supreme Court in 2015 after the court voted to uphold key tax subsidies that are part of the Affordable Care Act. But federal taxes and other measures designed to pay for the health care the ACA provides have not fared as well.
Andrew Harrer/Bloomberg via Getty Images
hide caption
toggle caption
Andrew Harrer/Bloomberg via Getty Images
It was a moment of genuine bipartisanship at the House Ways and Means Committee in October, as Democratic and Republican sponsors alike praised a bill called the “Restoring Access to Medication Act of 2019.”
The bill, approved by the panel on a voice vote, would allow consumers to use their tax-free flexible spending accounts or health savings accounts to pay for over-the-counter medications and women’s menstrual products.
Assuming the measure ultimately finds its way into law, it would also represent the latest piece of the Affordable Care Act’s financing to be undone.
Over-the-counter medication had been eligible to be considered a pretax expenditure in this way, before the ACA. But that eligibility was eliminated as part of a long list of new taxes and other measures that were designed to generate revenue to help pay for expanding health coverage to more people — a roughly $1 trillion cost of the health law over its first 10 years.
“It is paid for. It is fiscally responsible,” said President Barack Obama as he signed the ACA into law in 2010.
But not so much anymore. Many of the taxes and other provisions aimed at paying for that expanded health coverage “have been eliminated, delayed or are in jeopardy,” says Marc Goldwein of the Committee for a Responsible Federal Budget, a nonpartisan budget watchdog group. “All this stuff, it turns out, is very unpopular.”
The first piece of financing to disappear happened before most of the law even took effect. In 2011, Congress repealed a requirement that small businesses report to the IRS any payment of more than $600 to a vendor. The idea was that if more such payments were reported to taxing authorities, more taxes due on that income would actually get paid.
But small businesses complained — loudly — that the new paperwork requirement would be excessive, and Congress (and Obama) eventually agreed. The change alone eliminated an estimated $17 billion in ACA financing over 10 years.
Next, in 2015, Congress delayed (for the first time) the “Cadillac tax,” a 40% tax on the most generous employer health plans; one goal of that tax had been to curb excessive use of medical services.
That congressional delay came after intense lobbying by a coalition of business, labor and patient advocacy groups that banded together in a group called the Alliance to Fight the 40. It first got Congress to delay the Cadillac tax’s implementation from 2018 to 2020, then further pushed that date to 2022. And this past summer the House voted overwhelmingly to altogether eliminate the tax, which had been estimated to raise nearly $200 billion over the next decade.
Also on ice, thanks to that 2018 bill, are levies that were supposed to be paid by medical-device makers and health insurance companies, originally worth a combined $80 billion in financing during the law’s first decade.
Yet another — albeit fairly small — source of financing for the law went away in the 2017 GOP tax bill, which zeroed out the tax penalty for failing to have health insurance. The penalty raised $4 billion in 2018, the last year it was in effect.
Now it should be pointed out that the two ACA taxes that generate the most revenue are still on the books and collecting money. They are aimed at people with high incomes (more than $200,000 for individuals and $250,000 for couples) and were estimated to bring in more than $200 billion from 2010 to 2019. The measures, which don’t deal directly with services or provisions of the ACA, raise Medicare taxes on people at those higher incomes and increase taxes on unearned income.
The durability of those two taxes does not surprise Goldwein. Some are “unpopular to repeal,” he says, like “a tax on the rich that funds Medicare.”
What Goldwein does find surprising, though, is how durable some of the ACA’s other financing measures — reductions in spending — have been. For example, the health law, somewhat controversially, reduced Medicare payments to hospitals, insurance companies and a broad array of other health providers.
“The Medicare cuts have been for the most part surprisingly sustainable politically,” Goldwein says. Even when the GOP took over the House in 2011, its budget maintained the reductions from the ACA. So did the 2017 GOP “repeal and replace” proposal.
On the other hand, the appointed board of experts that was to rein in future Medicare spending, the “Independent Payment Advisory Board,” never got off the ground. Congress formally repealed it in 2018.
So what does this all mean? The past decade has shown that it has been relatively easy to make hard-won tax increases go away, suggesting that interest groups — particularly health industry groups representing drugmakers, insurers and hospitals — still wield a lot of power on Capitol Hill.
“Right now, everyone wants to cancel a 3% tax on the health insurance industry,” he says, referring to the current efforts of a major ad campaign by a coalition of small-business owners and insurance groups to get Congress to delay or cancel that ACA-linked tax.
Given how much money from health insurers is going into fighting that tax, he says, how likely is it that Congress — even one controlled by Democrats — would really “cancel the whole industry” by passing a “Medicare for All” bill?
Kaiser Health News is a nonprofit, editorially independent program of the Kaiser Family Foundation. KHN is not affiliated with Kaiser Permanente.